here - Wellbeing Clinic
advertisement

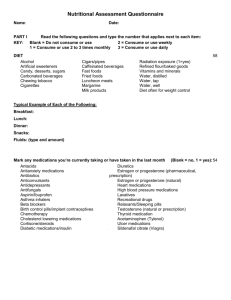
Naturopathic Health Questionnaire “treat the whole; affect the mind; lift the spirit” Sarah Couchman ND BSc D.O Sp Dip Naturopath The Wellbeing Clinic 1 Windmill Road Headington Oxford OX3 7BL The following questionnaire will help to gather information about your health history and current health status. Please take the time to answer questions as accurately as possible and return to me at the address below prior to your consultation. Your appointment will last between 1 and 1 1/2 hours so that further clinical assessments any questions can be answered fully. Please endeavour to arrive on time for your appointment. If, for any reason, you need to reschedule your appointment, please inform myself directly or contact the clinic on the number below at the earliest convenience, this will avoid a cancellation charge. Cancellation fee of full payment will be charged when a cancellation is made with less than 48 hours notice. This ensures other clients are able to use the appointment time. Enquiries: 01865 751111 Mobile: 07810354407 Private and Confidential First Name: Last Name: Address: Email Address: Tel: Mobile: Date of Birth: Occupation: Weight: Height: GP: GP Surgery: Please list current medical complaints in order of severity: Symptoms Length of time this has been happening 1 2 3 4 Please list any medication you are currently taking (include contraceptive pill, herbs, vitamins, minerals etc) Medication 1 2 3 4 Dose (if known) Length of time you have been taking this medication Heredity Profile What illnesses are/were the following prone to? Your Father Your Mother Your Siblings Your Children What illnesses did you have as a child? (e.g. Measles, Polio, Ear Infections, Mumps, Chicken Pox, Appendicitis, German Measles, Tonsilitis) Did you reject milk or any other foods as a child? Do you have any known allergies? Please list: Do you suffer frequent colds/viruses/infections? Yes No Have you been diagnosed with any illnesses? (e.g. IBS, colitis, hernia) Do you have gum disease or any other dental/mouth problems? Have you had any operations including removal of organs? Please give approximate dates. How frequently do you move your bowels? Daily Following meals Infrequently Are stools easy to pass? Yes No: is this a recent problem and/or associated with other problem (e.g. piles)? Have you noticed blood or mucus in your stools? Recently In the past Lifestyle Are you under any stress at the moment? Yes No If yes, are these stressors related to your health or environmental/social factors? Do you work more than 60 hours per week? Yes No Are you especially competitive? Yes No Do you feel you worker harder than most people you know? Yes No Are you exposed to chemicals at work? Yes No If yes, please give details: How much time per day do you spend in front of a screen (TV/VDU)? Do you spend more than 2hrs a week driving? Yes No Do you smoke more than 5 cigarettes per day? Yes No Do you live or work in a smoky atmosphere? Yes No Do you drink over 1 unit of alcohol per day? Yes No What do you prefer to drink? Wine Beer Spirits Do you easily become angry? Yes No How many times do you exercise per week? Is your energy less now than it used to be? Yes No Do you feel guilty when relaxing? Yes No Are you unclear about your goals in life? Yes No Do you have difficulty getting to sleep? Yes No How would you describe your emotional character? Have you suffered from significant bereavement/severe trauma/separation in the last 5 years? Have you had any accidents? (e.g. falls, car accidents, broken bones) What makes your problems better or worse? Nutritional Profile Please tick the food groups you eat every day and answer following questions: Meat (Fish, beef, lamb, pork, turkey, chicken) -how many times per week do you eat white meat (fish or poultry)? -how many times per week do you eat red meat (beef, pork, lamb or game)? Dairy (milk, cheese, yoghurt) -how many pints per week? -what type of milk? Vegetables and fruit (any fruit, green or yellow vegetables) -do you wash fruit and vegetables before preparing/eating? Cereals (bread, biscuits, cooked or cold cereal) -do you normally eat white rice or products made with white flour? -how much bread or rolls do you eat per day? Please indicate the amount you have of the following: Per day Cups of tea or coffee Sugar in tea or coffee Adding salt to food Snacks Per week Fast food Canned or frozen food Fried food (chips etc) Chocolate/sweets What snacks do you eat during the day? (e.g. crisps, nuts, dried fruit, biscuits) Do you use a water filter or drink bottled water instead of tap water? Do you frequently eat under stressed conditions or on-the move? Does your job involve eating out a lot? How would you describe your appetite? Please shade the following on the clock-faces below: a) Fatigue: when you feel fatigue during the day b) Energy: when you have the most energy c) Sleep: when you fall asleep, when you wake, include naps. AM PM Specific Symptoms Please tick the problems you have experienced in the last month, as well as indicating whether these have been an issue in the past. Belching or gas within 1 hr of eating Heartburn acid reflux Bloating after eating Bad breath Using indigestion tablets Feeling excessively full after eating Eating quickly Anaemia (unresponsive to iron) Pain between shoulder blades Nausea Stomach upset by greasy foods Brown spots on skin Light or clay-coloured stools Chronic fatigue or Fybromyalgia Upper Gastrointestinal System Current Past Feeling like skipping breakfast Feeling sleepy after meals Chipped/easily broken nails Stomach pains/cramps Feeling better if you don’t eat Upset stomach after taking vitamins Diarrhoea after meals Undigested food in stools Liver and Gallbladder Current Past Drug or alcohol use in response to stress Hepatitis Long term use of prescription medications Easily intoxicated by alcohol Hurried eating habits Sensitive to chemicals (e.g. perfume, solvents, insecticides, car exhausts) Current Food alleries Abdominal bloating 1-2 hrs after eating Specific foods make you tired or bloated Pulse speeds up after eating Airborne allergies (e.g. hayfever) Current Never get sick Runny nose Cough producing mucus Frequent infections: ear, sinus, lung, skin, bladder Small Intestine Past Hives Asthma, sinus infection, stuffy nose Sometimes feel “spacey” or unreal Alternating constipation and diarrhoea Feeling as though there are foods you cannot give up Immune system Past Itchy skin or dermatitis Cysts, boils or rashes Frequent colds or flu Epstein Bar, Mono, herpes, shingles, chronic fatigue Current Past Current Past Current Past Current Past Current Heavy breathing High cholesterol Family history of heart disease Dizziness Short of breath on exertion Blood pressure above 140/90 Discomfort at high altitudes Fluid retention (e.g. swollen ankles) Current Insomnia Slow starter in the morning Feel wired or jittery when drinking coffee Clench or grind teeth Calm on the outside, troubled on the inside Become dizzy on standing Increased sex drive Weight gain around face, waist and hips Adrenal Past Crave salty foods Muscles easily fatigued Chronic fatigue, or feel drowsy Afternoon yawning Afternoon headache Current Past Current Past Current Past Allergies/hives Loss of appetite Current Flush easily/sweat with little activity Difficulty gaining weight, even with large appetite Nervous, emotional, can’t work under pressure Inward trembling Allergic to iodine Intolerance to high temperatures Fast pulse even when rested Diarrhoea Facial, limb laryngeal muscle spasm Nausea, vomiting Increased urination Cardiovascular Past Overweight Seldom exercise vigorously Smoke, drink use recreational drugs Muscle cramp during exercise Problems with breathing Tension or tightness under breastbone, worse on exertion Respiratory problems Dull chest pain which may radiate to left arm Thyroid Past Mentally sluggish, reduced initiative Easily fatigued, sleep during the day Sensitive to cold – poor circulation Chronic constipation Difficulty losing weight Loss of lateral third of eyebrow Seasonal sadness Thinning hair Twitching Anaemia Loss of appetite Increased thirst Current Wake after a few hours’ sleep, hard to get back to sleep Cuts and bruises take a long time to heal Eat desserts/sugary snacks Binge or uncontrolled eating Excessive appetite Crave coffee or sugar in the afternoon Sleepy in the afternoon Decreased sugar tolerance Sugar Balance Past Fatigue that is relieved by eating Past Current Past Current Past Current Past Headaches if meals are skipped or delayed Irritable before meals Shaky if meals are delayed Frequent thirst Family members with diabetes Frequent urination Crave sweets Experience PMS/PMT Infertility Poor memory/ concentration Essential Fatty Acids Current Past Dry eyes Excessive thirst or sweating Dry, flaky skin or dandruff Vulnerable to insect bites Numbness/itching/tingling in extremities Depressed Pale skin Easily exhausted Teeth grinding Unable to remember dreams Small bumps on back of arms Decreased sense of smell/taste White spots on fingernails Strong food odour Vitamin and Mineral Needs Current Past Sore tongue Worrying, apprehensive, anxious Muscles easily fatigued Slow wound healing Bone loss MSG sensitivity Take contraceptive pill Sensitive to strong light at night Bleeding gums, especially when brushing teeth Muscle cramps Nosebleeds, bruise easily Current Prostate problems Difficulty starting/stopping urine stream Pain or burning on urinating Pain on inside of legs/heels Sensation of incomplete bowel evacuation Melancholia Current Men only Past Decreased sexual function Waking regularly at night to urinate Chronic constipation Low energy, tire easily Nervousness in legs especially at night Current Depression during periods Breast fibroids – benign masses Crave chocolate around periods Excess facial or body hair Excessive menstrual flow Minimal menstrual blood flow Occasional skipped periods Water retention Thrush Problems with pregnancy Post menopausal Women only Past Mood swings (PMS) Breast tenderness associated with cycle Vaginal discharge/itchiness/cystitis Vaginal dryness Hot flushes Endometriosis Uterine fibroids Bloating Trying to conceive Symptoms of menopause Taking HRT Current Past While this questionnaire is very comprehensive, there may be problems or issues yet raised, which you feel are relevant to your assessment. Please outline any other issues not covered: Thank you for taking the time to fill in the questionnaire, please return it with your deposit to Sarah Couchman 30 Beaumont Street Oxford OX1 2NY. Sarah Couchman ND BSc DO Naturopath Mob: 07810354407