HEALTH HISTORY FORM Name: What do you like to be called
advertisement

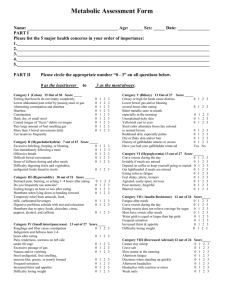
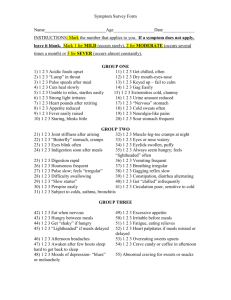
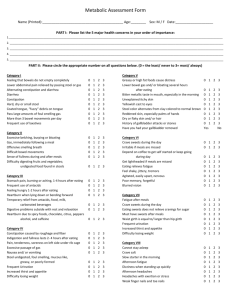
HEALTH HISTORY FORM Name:_______________________________ What do you like to be called?__________ Full Address, City, State, Zip:________________________________________________ ________________________________________________________________________ May we send mail to this address? _____ Best Contact Number(s): ___________________________________________________ May we leave messages at this number? _____ Email Address:______________________________ (Handouts for sessions will be sent to the email address you provide.) Age: _____ Height: _____ Date of Birth: ___________Place of Birth: _______________ Current Weight: _______ Weight 6 Months Ago: _______ Weight 1 Year Ago: _______ Would you like your current weight to be different? If so, what? ___________________ Relationship Status: ___________________ Children: ___________________________ Pets:____________________________________ Occupation: ____________________ Hours of work per week: ________ Hobbies: ___________________________________ Top 5 things you would like to change in order of importance to YOU (please be specific): _______________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ At what point in your life did you feel your best and why? ________________________________________________________________________ Any diagnosed illnesses/hospitalizations/injuries? ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ Ancestry: ______________________________ Blood Type: __________ Do you sleep well? _______ How many hours? _______ Do you wake up at night? ____ If yes, why? _____________________________________________________________ Any pain, stiffness, or swelling? _____________________________________________ Constipation, diarrhea, gas, heartburn, irregularity, or indigestion? Please explain: ________________________________________________________________________ ________________________________________________________________________ Allergies or sensitivities (including environmental, food, and drugs)? Please explain: ________________________________________________________________________ ________________________________________________________________________ Supplements and/or medications: ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ Involved with any other alternative healers or therapists? ________________________________________________________________________ What role do sports and/or exercise play in your life? ________________________________________________________________________ Please list your typical daily diet: Breakfast: _______________________________________________________________ Lunch: _________________________________________________________________ Dinner: _________________________________________________________________ Snacks: _________________________________________________________________ Liquids: ________________________________________________________________ What percentage of your food is home-cooked? ______ Who cooks? ________________ Where does the rest come from? _____________________________________________ Do you crave sugar, coffee, caffeine, cigarettes, or have any other addictions? ________________________________________________________________________ Anything else you would like to share? ________________________________________________________________________ ________________________________________________________________________ Women Only: Are you periods regular? ____ How many days is your flow? ____ How frequent? ____ Painful or symptomatic? Please explain: ______________________________________ Reached or approaching menopause? _________________________________________ Birth Control History: _____________________________________________________ Do you experience yeast infections or urinary tract infections? Please explain: ________________________________________________________________________ Symptom Survey ________________________________________________________________________ For Health Counselor’s Use Only Blood Pressure Sitting _____/_____ Blood Pressure Standing_____/_____ Heart Rate _______ BPM ________________________________________________________________________ Please fill out the form below. If the symptom does not apply to you, you do not have to fill out anything for that symptom. If it does apply to you, please put “1” for mild (occurs rarely), “2” for moderate (occurs several times a month), and “3” for severe (occurs almost constantly). Some symptoms may repeat among groups, but it is important to complete the entire form. GROUP 1 Acid foods upset __ Get chilled often __ Lump in throat __ Dry mouth, eyes, or nose __ Pulse speeds after meals __ Failure to calm down __ Cuts heal slowly __ Gag easily __ Startles easily __ Extremities cold and/or clammy __ Strong light irritates __ Urine amount reduced __ Heart pounds after retiring __ Nervous stomach __ Appetite reduced __ Cold sweats __ Fever easily __ Neuralgia (nerve pain) __ Blinks little, stares often __ Sour stomach __ GROUP 2 Joint stiffness upon rising __ Muscle, leg, toes cramps at night __ Butterfly stomach __ Eyes and/or nose watery __ Eyes blink often __ Eyelids puffy __ Indigestion soon after meals __ Always hungry __ Digestion rapid __ Vomiting frequent __ Hoarseness frequent __ Breathing irregular __ Pulse slow __ Gagging reflex slow __ Difficulty swallowing __ Constipation/diarrhea alternating __ “Slow starter” __ Get chilled frequently __ Perspire easily __ Circulation poor __ Subject to colds, asthma, bronchitis __ GROUP 3 Eat when nervous __ Excessive appetite __ Hungry between meals __ Get shaky if hungry __ Fatigue, eating relieves __ Lightheaded if meals delayed __ Heart palpitates if meals delayed __ Afternoon headaches __ Overeating sweets causes illness __ Awaken after few hours of sleep __ Crave candy, coffee, soda in afternoon __ Moods of depression __ Abnormal cravings for sweets or snacks __ GROUP 4 Hands and feet go to sleep easily __ Sigh frequently __ Aware of breathing heavily __ High altitude discomfort __ Susceptible to colds and fevers __ Afternoon yawner __ Get drowsy often __ Swollen ankles __ Charley horses __ Shortness of breath upon exertion __ Dull pain in chest radiating to left arm __ Bruise easily __ Tendency to anemia __ Nose bleeds frequent __ Ringing in ears __ Tightness in chest __ GROUP 5A Dizziness __ Dry skin __ Burning feet __ Blurred vision __ Itching skin and feet __ Excessive hair loss __ Frequent skin rashes __ Bitter, metallic taste in mouth __ Bowel movements painful or difficult __ Worrier __ Headache over eyes __ GROUP 5B Greasy foods upset __ Stools light colored __ Skin peels on foot soles __ Pain between shoulder blades __ Use laxatives __ Stools alternate from soft to watery __ History of gallbladder issues __ GROUP 5C Sneezing attacks __ Nightmares __ Bad breath __ Milk products cause distress __ Sensitive to hot weather __ Burning or itching anus __ Crave sweets __ GROUP 6A Loss of taste for meat __ Lower bowel gas several hours after eating __ Burning stomach sensations, eating relieves __ GROUP 6B Coated tongue__ Pass large amounts of foul-smelling gas __ Indigestion ½-1 hours after eating __ GROUP 6C Irritable bowel __ Gas shortly after eating __ Stomach bloating after eating __ GROUP 7A Insomnia __ Nervousness __ Can’t gain weight __ Intolerance to heat __ Highly emotional __ Flush easily __ Night sweats __ Thin, moist skin __ Inward trembling __ Heart palpitations __ Increased appetite without weight gain __ Pulse fast at rest __ Eyelids and/or face twitch __ Irritable and restless __ Can’t work under pressure __ GROUP 7B Increase in weight __ Decrease in appetite __ Fatigue easily __ Ringing in ears __ Sleepy during day __ Sensitive to cold __ Dry or scaly skin __ Constipation __ Mental sluggishness __ Hair coarse __ Headaches upon rising __ Slow pulse (below 65) __ Frequent urination __ Impaired hearing __ Reduced initiative __ GROUP 7C Failing memory __ Low blood pressure __ Increased sex drive __ Headaches __ Decreased sugar tolerance __ GROUP 7D Abnormal thirst __ Bloating of abdomen __ Weight gain around hips or waist __ Sex drive reduced __ Tendency to ulcers and/or colitis __ Increased sugar tolerance __ Women: Menstrual irregularity __ GROUP 7E Dizziness __ Headaches __ Hot flashes __ Increased blood pressure __ Hair growth on face of body (female) __ Sugar in urine without diabetes __ GROUP 7F Weakness __ Chronic fatigue __ Low blood pressure __ Nails weak ridged __ Tendency to hives __ Arthritic tendencies __ Perspiration increased __ Bowel disorders __ Poor circulation __ Swollen ankles __ Crave salt __ Brown spots or bronzing on skin __ Allergies __ Tendency to asthma __ Respiratory disorders __ GROUP 8 Apprehension __ Irritability __ Morbid fears __ Never seems to get well __ Forgetfulness __ Indigestion __ Poor appetite __ Craving for sweets __ Muscular soreness __ Depression __ Noise sensitivity __ Acoustic hallucinations __ Tendency to cry for no reason __ Skin sensitive to touch __ Anorexia __ Bulimia __ Inability to concentrate __ Frequent stuffy nose __ Loose joints __ Acne __ Urination difficult, dribbling __ Night urination __ Feeling of incomplete bowel evacuation __ Leg nervousness __ Taunya Bruton, H.C., BSc. Certified Health Counselor Phone: 540-381-6215 Fax: 540-381-6216 taunya@lifeinbalancecenter.com www.truewealthishealth.com www.lifeinbalancecenter.com