Appendix 1 EHC Client Record Form 23.4.15
advertisement

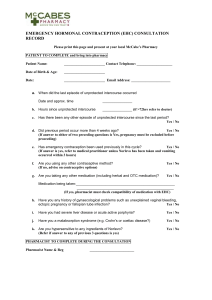
Appendix 1: Pharmacy Client Record for the Community Pharmacy Emergency Hormonal Contraception Service and Chlamydia Testing Service Pharmacy Stamp Client’s Details Client name/initials (FULL NAME IF CONSENT GIVEN TO FOLLOW UP REFERRAL) Date of consultation Age/ DoB Post Code Contact telephone number for referral to follow up advice Date of 1st day of LMP Length of normal menstrual cycle Day of cycle of UPSI Reason for request Please tick box UPSI Missed pill Condom failure Vomiting/diarrhoea Antibiotic/drug therapy Other (please state) Please state where client heard about scheme: Criteria for Inclusion for EHC Has client missed her contraceptive pill? Advice given if missed contraceptive pill? Since LMP, client has only had unprotected intercourse within the last 72 hour period? All options for emergency contraception discussed: Leaflet EHC IUCD Client accepts hormonal method Criteria for referral (exclusion) for EHC Client is under 12 years Client is under 13 years Yes No Yes No N/A Action EHC cannot be supplied and mandatory reporting to social services – Child protection issue EHC supply for those aged 12 and over only and mandatory reporting to Social Services – Child protection issue Client is under 16 years - Use Fraser Guidelines Has the client used any other form of emergency contraception within this cycle? Was her last period more than 4 weeks ago? Is the client pregnant or likely to be pregnant? Was last period abnormal in anyway? Did UPSI occur more than 72 hours ago? Does client have known hypersensitivity to levonorgestrel/excipient? Is client on any other medication? Does client have acute severe liver disease? Does client have acute active porphyria? Does client have severe malabsorption syndromes? Refer to social services if concerns identified If yes refer, but if Levonelle has been taken and vomited refer to guidance If yes, carry out pregnancy test/refer If yes, refer to Family planning clinic or GP If yes, refer to Family planning clinic or GP If yes, refer to Family planning clinic or GP If yes, refer to Family planning clinic or GP Check BNF for interactions If yes, refer to Family planning clinic or GP If yes, refer to Family planning clinic or GP If yes, refer to Family planning clinic or GP Counselling/Actions Yes Mode of action and effectiveness including failure rate discussed Side effects Possible effects on foetus Follow up Condoms issued Sexual Health advice given Leaflets given (EHC, Contraception, GUM clinics) Future contraception discussed Give leaflet on LARC available http://guidance.nice.org.uk/CG30/PublicInfo/PrintFriendly/doc/English Chlamydia discussed including risks of contracting, signs and symptoms Client is eligible for Chlamydia screening kit Chlamydia screening kit given out Referral to Follow up Advice Action Taken Supply: Levonelle 1500 Batch number and expiry date Referral Yes/no No (If further advice is required, contact any of the support centres or refer client to any Family Planning Clinic or GP.) The above information is correct to the best of my knowledge. I have been counselled on the use of emergency contraception; Chlamydia and the screening programme and understand the advice given to me. On this occasion I accept/decline (please delete as appropriate) the Chlamydia screening kit. I agree/disagree (please delete as appropriate) to be contacted by the Community and Sexual Health services three weeks from the date of this consultation. Clients Signature Date The action specified was based on the information given to me by the client, which, to the best of my knowledge, is correct. Pharmacists Signature Date PLEASE KEEP THIS FORM AT THE PHARMACY AS A RECORD AND FAX THIS FORM TO C&SH WILLENHALL HEALTH CENTRE, FIELD STREET 01922 604823