DSRIP Plan: UC Davis Medical Center Page CATEGORY 1
advertisement

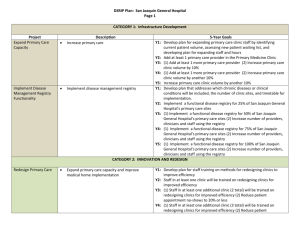
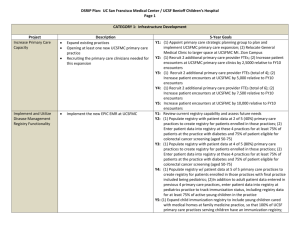
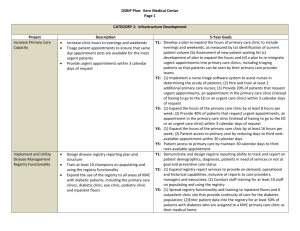
DSRIP Plan: UC Davis Medical Center Page 1 CATEGORY 1: Infrastructure Development Project Implement and Utilize Disease Management Registry Functionality Collection of Accurate Race, Ethnicity and Language (REAL) Data to Reduce Disparities Description expand chronic disease management programs in the ambulatory setting design care coordination strategies to optimize care across a continuum incorporate decision-support for chronic disease management into team-based practice 5-Year Goals Y1: (1) develop a plan (identify current patient volume, assess new patients with chronic disease diagnoses, plan expansion of services and sites, plan expansion of current programs to all primary care clinics); (2) develop patient experience metric question; (3) use paper-based companion survey for on-site clinic use Y2: (1) implement system to manage newly diagnosed chronic disease patients at 1 primary care clinic; (2) develop tethered registry to capture patient enrollment in chronic disease management program; (3) design patient experience report Y3: (1) expand chronic disease management program team to 2 additional clinic sites; (2) implement tethered registry for chronic disease management; (3) compare patient experience metric against team integration at sites Y4: (1) expand chronic disease management program/registry team to at least 4 additional clinic sites; (2) compare patient experience metric against team integration at sites Y5: (1) expand chronic disease management program/registry team to at least 6 additional clinic sites; (2) compare patient experience metric against team integration at sites Develop ability to collect patient demographic data that can be compared to quality and health outcomes data Stratify patient, demographic data by outcomes to identify disparities engage in quality improvement projects to reduce health care disparities Y1: (1) develop Ambulatory plan to assess collection of REAL data; 92) report on preliminary REAL data collection Y2: (1) develop plan to stratify patient outcomes using REAL data and strategy to link to quality data; (2) patient experience questionnaire to be designed and tested using sample set of patients across demographics Y3: (1) Record designated REAL data fields for at least 50% of unique patients; (2) analyze Patient experience questionnaire Y4: (1) Record designated REAL data fields for at least 70% of unique patients; (2) analyze patient experience questionnaire Y5: (1) Record designated REAL data fields for at least 90% of unique patients; (2) perform REAL data analysis and identify at least 2 specific health care disparities; (3) analyze patient experience questionnaire DSRIP Plan: UC Davis Medical Center Page 2 CATEGORY 2: INNOVATION AND REDESIGN Implement/Expand Care Transitions Program Conduct Medication Management Create mechanism to identify within the emergency department and track in all settings, patients with specific chronic diseases create “intensive care management” (ICM) registry and management system increase staffing in the ED to provide ICM optimize patients’ medications prior to discharge reconcile medications at time of discharge provide after-discharge follow-up provide patient education configure alerts within EHR to ensure outpatient prescriptions comply with criteria for use of Black Box warning medications fully implement bedside barcode scanning and smart infusion pumps Y1: Y2: Y3: Y4: Y5: Y1: Y2: Y3: Y4: Y5: Expand Medical Homes expand preventive immunizations programs design care coordination strategies incorporate decision-support for immunization prevention and wellness education into teambased practices Y1: Y2: Y3: expand current ICM within the ED (hire 2 additional Care Managers) expand ED case management to 7 days/week (4 case management FTEs 10 hours/day) implement ICM registry and use it for more than 50% of all ED casemanaged patients and for all patients admitted from ED into hospital implement ICM egistry use it for more than 90% of all ED casemanaged patients and for all patients admitted from ED into hospital (blank) (1) implement pilot of bedside barcode scanning (2) initiate implementation of smart infusion pumps (1) implement services to improve continuity of medication use for patients with heart failure or on warfarin (hire pharmacist and nurse and provide continuity of medication use services to at least one patient); (2) provide services to improve continuity of medication use to at least 50% of patients with heart failure or on warfarin; (3) implement safeguards in EHR to ensure compliance with criteria for safe use of Black Box Warning medications; (4) implement more smart infusion pumps; (5) complete planning for full implementation of bedside barcode scanning (1)provide services to 75% of heart failure and warfarin patients; (2) implement clinical pharmacist services for COPD pneumonia and AMI patients; (3) fully implement bedside barcode scanning of medications provide clinical pharmacist services to 75% of heart failure and warfarin patients and 50% of COPD, pneumonia and AMI patients provide clinical pharmacist services to 75% of all targeted patients (1) develop timeline and plan to submit application for Patient Centered Medical Home (PCMH) recognition by NCQA; (2) apply for at least one primary care site; (3) develop plan to identify new and existing ambulatory patients requiring influenza vaccination (1) develop timeline and plan for submission of PCMH application for primary care sites; (2) develop patient experience survey using PCMH criteria; (3) design seasonal influenza notification system; (4) design MyChart influenza notification report for provider use (1) develop plan for submission of PCMH application for remaining primary care sites; (2) develop plan and timeline to implement Apply Process Improvement Methodology to Improve Quality/Efficiency DSRIP Plan: UC Davis Medical Center Page 3 patient experience survey in remaining sites; (3) develop plan to integrate influenza vaccination at all primary care sites Y4: (1) develop timeline and plan to submit application for PCMH recognition for hospital-based primary care clinics; (2) develp PCMH Patient Experience Focus Groups; (3) develop EHR report for provider, buy site and provider, on influenza vaccination rate Y5: (1) assign at least 40% of eligible patients to PCMH medical homes; (2) report shared learning of medical home model; (3) develop plan for ongoing patient engagement through Patient Experience Board; (4) develop EHR rport for specialty care providers who provide influenza vaccines, by site and provider, on influenza vaccination rates Using Lean Six Sigma: Y1: (1) develop designated unite responsible for Lean Six Sigma implementation and assess processes; (2) LSS Just-in-time training to identify and eliminate waste within health care at least 2 multidisciplinary teams for specific projects delivery value system Y2: (1) develop early-warning systems within EHR to act on identified install mistake-proofing systems problems; (2) LSS Just –in-Time training to at least 2 multidisciplinary shift culture from accepting errors and defects to teams for specific projects trusting a perfect patient experience is possible Y3: (1) continue to use and further develop early-warning systems in the maximize the use of tools EHR; (2) LSS Master Black Belts provide 4 LSS Green Belt courses per focus on reducing selected HACs year; (3) LSS Just –in-Time training to at least 2 multidisciplinary teams for specific projects Y4: (1) continue to use and further develop early-warning systems in the EHR; (2) LSS Master Black Belts provide 4 LSS Green Belt courses per year; (3) LSS Just –in-Time training to at least 2 multidisciplinary teams for specific projects Y5: (1)real-time alerts of patient errors and problems; (2) LSS Master Black Belts provide 4 LSS Green Belt courses per year; (3) LSS Just – in-Time training to at least 2 multidisciplinary teams for specific projects CATEGORY 4: URGENT IMPROVEMENT IN CARE Improve Severe Sepsis Detection and Mangement implement Sepsis Management and Resuscitation Bundle Y1: Y2: (1) join Sepsis Improvement Collaborative and join Foundation to learn and share best practices; (2) convene multi-disciplinary group to develop goals and work plans for reducing severe sepsis; (3) use Lean Six Sigma to optimize efficiencies in evaluating and implementing improvement project (1) implement best practice alerts within EHR for early sepsis Central Line Associated Blood Stream Infection (CLABSI) Prevention Surgical Site Infection DSRIP Plan: UC Davis Medical Center Page 4 recognition; (2) report at least 6 months of data to SNI; (3) report results to State Y3: (1) achieve TBD% compliance with sepsis resuscitation bundle; (2) share data and practices with SNI for benchmarking; (3) report results to State Y4: (1) achieve TBD% compliance with sepsis resuscitation bundle; (2) share data and practices with SNI for benchmarking; (3) report results to State Y5: (1) achieve TBD% compliance with sepsis resuscitation bundle; (2) share data and practices with SNI for benchmarking; (3) report results to State Y1: implement Central Line Insertion Practices (CLIP) improve compliance with central line insertion Y2: (1) report 6 months of data on CLIP to SNI; (2) report 6 months of bundle data to CLABSI to SNI; (3) report CLIP results to State Y3: (1)achieve TBD% compliance with CLIP; (2) share data and practices with SNI; (3) report CLIP and CLABSI results to State Y4: (1) achieve TBD% compliance with CLIP; (2) reduce central line bloodstream infections by TBD%; (3) share data and practices with SNI; (4) report CLIP and CLABSI results to State Y5: (1) achieve TBD% compliance with CLIP; (2) reduce central line bloodstream infections by TBD%; (3) share data and practices with SNI; (4) report CLIP and CLABSI results to State improve surgical site infection prevention Y1: Y2: Y3: Y4: Y5: Hospital-acquired Pressure Ulcer (HAPU) Prevention use a multi-disciplinary team approach to the prevention of pressure ulcers using evidencebased recommendations from the national Pressure Ulcer Advisory Panel Y1: Y2: Y3: (1) Validate TheraDoc software to streamline SSI surveillance; (2) establish SSI baseline for reporting (1) Install TheraDoc software and train staff; (2) report at least 6 months of data on SSI to SNI; (3) report results to State (1) reduce rate of SSI for Class I and 2 wounds by TBD rate; (2) share data and practices with SNI; (3) report results to the State (1) reduce rate of SSI for Class I and 2 wounds by TBD rate; (2) share data and practices with SNI; (3) report results to the State (1) reduce rate of SSI for Class I and 2 wounds by TBD rate; (2) share data and practices with SNI; (3) report results to the State (1) implement EHR template for SWAT team for documentation of skin assessment; (2) develop electronic dashboard to measure and report/share HAPU prevalence to inpatient units (1) share data and findings with SNI; (2) report results to the State (1) achieve HAPU prevalence of less than 2.0%; (2) share date and DSRIP Plan: UC Davis Medical Center Page 5 findings with SNI; (3) report results to State Y4: 1) achieve HAPU prevalence of less than 1.5%; (2) share date and findings with SNI; (3) report results to State Y5: 1) achieve HAPU prevalence of less than 1.1%; (2) share date and findings with SNI; (3) report results to State