DSRIP Plan: San Joaquin General Hospital Page CATEGORY 1
advertisement

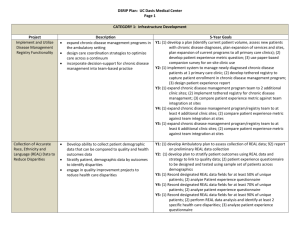
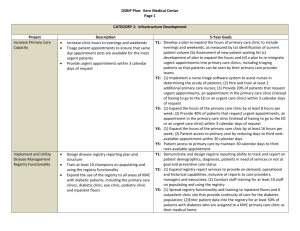
DSRIP Plan: San Joaquin General Hospital Page 1 CATEGORY 1: Infrastructure Development Project Expand Primary Care Capacity Implement Disease Management Registry Functionality Redesign Primary Care Description Increase primary care 5-Year Goals Y1: Develop plan for expanding primary care clinic staff by identifying current patient volume, assessing new patient waiting list, and developing plan for expanding staff and hours Y2: Add at least 1 primary care provider in the Primary Medicine Clinic Y3: (1) Add at least 1 more primary care provider (2) Increase primary care clinic volume by 10% Y4: (1) Add at least 1 more primary care provider (2) Increase primary care clinic volume by another 10% Y5: Increase primary care clinic volume by another 10% Y1: Develop plan that addresses which chronic diseases or clinical Implement disease management registry conditions will be included, the number of clinic sites, and timetable for implementation. Y2: Implement a functional disease registry for 25% of San Joaquin General Hospital’s primary care sites Y3: (1) Implement a functional disease registry for 50% of San Joaquin General Hospital’s primary care sites (2) Increase number of providers, clinicians and staff using the registry Y4: (1) Implement a functional disease registry for 75% of San Joaquin General Hospital’s primary care sites (2) Increase number of providers, clinicians and staff using the registry Y5: (1) Implement a functional disease registry for 100% of San Joaquin General Hospital’s primary care sites (2) Increase number of providers, clinicians and staff using the registry CATEGORY 2: INNOVATION AND REDESIGN Expand primary care capacity and improve medical home implementation Y1: Develop plan for staff training on methods for redesigning clinics to improve efficiency Y2: Staff in at least one clinic will be trained on redesigning clinics for improved efficiency Y3: (1) Staff in at least one additional clinic (2 total) will be trained on redesigning clinics for improved efficiency (2) Reduce patient appointment no-shows to 20% or less Y4: (1) Staff in at least one additional clinic (3 total) will be trained on redesigning clinics for improved efficiency (2) Reduce patient DSRIP Plan: San Joaquin General Hospital Page 2 appointment no-shows to 15% or less Y5: Reduce patient appointment no-shows to 20% or less Train primary care clinic staff so that at least 1000 Y1: Develop plan Y2 : Develop medical home assignment criteria, including which specific patients in primary care clinics are assigned to chronic conditions, high risk patients, and high utilization patients will medical homes be assigned to medical homes Y3: At least 400 eligible patients assigned to medical homes Y4: At least 750 eligible patients assigned to medical homes Y5: At least 1000 eligible patients assigned to medical homes CATEGORY 4: URGENT IMPROVEMENT IN CARE Expand Medical Homes Improve Severe Sepsis Detection and Management Central Line Associated Blood Stream Infection (CLABSI) Prevention improve compliance with central line insertion bundle Reduce avoidable harm or deaths and costs of care due to central-line associated blood stream infections Surgical Site Infection improve surgical site infection prevention implement Sepsis Management and Resuscitation Bundle Reduce avoidable harm or deaths due to severe sepsis to patients receiving inpatient services Y1: Develop plan. Y2: (1) Implement the Sepsis Resuscitation Bundle: (2) Report at least 6 months of data to SNI for baseline / benchmarks; (3) Report the results to the state. Y3: (1) achieve TBD% compliance with sepsis resuscitation bundle; (2) share data and practices with SNI for benchmarking across public hospitals; (3) Report results to the state Y4: (1) achieve TBD% compliance with sepsis resuscitation bundle; (2) share data and practices with SNI for benchmarking across public hospitals; (3) Report results to the state Y5: (1) achieve TBD% compliance with sepsis resuscitation bundle; (2) share data and practices with SNI for benchmarking across public hospitals; (3) Report results to the state Y1: Develop plan Y2: (1) Implement the Central Line Insertion Practices (CLIP; (2) Report at least 6 months of data collection on CLIP to SNI for baseline / benchmarks; (3) Report at least 6 months of data collection on CLABSI to SNI baseline / benchmarks; (4) Report CLIP results to the state Y3: (1)achieve TBD% compliance with CLIP; (2) share data and practices with SNI; (3) report CLIP and CLABSI results to State Y4: (1) achieve TBD% compliance with CLIP; (2) reduce central line bloodstream infections by TBD%; (3) share data and practices with SNI; (4) report CLIP and CLABSI results to State Y5: (1) achieve TBD% compliance with CLIP; (2) reduce central line bloodstream infections by TBD%; (3) share data and practices with SNI; (4) report CLIP and CLABSI results to State YI: Develop a plan to collect and report data about surgical site infections Y2: (1) Report at least 6 months of data to SNI for baseline/benchmark (2) Stroke Management DSRIP Plan: San Joaquin General Hospital Page 3 Report results to the state (3) Work with IT to capture patients with surgical site infections that are not readmitted or have their wound cultured Y3: (1) Reduce rate of SSI for Class 1 and 2 sounds by X, (X TBD in year 2) (2) Share data, promising practices and findings with SNI to foster shared learning and benchmarking across the California public hospitals (3) Report results to the state Y4: (1) Reduce rate of SSI for Class 1 and 2 sounds by X, (X TBD in year 2) (2) Share data, promising practices and findings with SNI to foster shared learning and benchmarking across the California public hospitals (3) Report results to the state Y5: (1) Reduce rate of SSI for Class 1 and 2 sounds by X, (X TBD in year 2) (2) Share data, promising practices and findings with SNI to foster shared learning and benchmarking across the California public hospitals (3) Report results to the state Improve stroke care to reduce unnecessary death Y1: Develop plan to identify, monitor and report about the seven stroke management process measures and harm and improve rehabilitation rates using Y2: (1) Report at least 6 months of data collection on the 7 stroke JCAHO and American Stroke Association management process measures to SNI (2) Report the data to the state guidelines Y3: (1) Increase rate of ischemic stroke patients prescribed antithombotic therapy at discharge by TBD (2) Increase rate of ischemic stroke patients with atrial fibrillation/flutter discharged on anticoagulant therapy by TBD (3) Increase rate of acute ischemic stroke patients who arrive at hospital within 120 minutes and for whom IV t-PA was initiated within 180 minutes by TBD (4) Increase rate of ischemic stroke patients who receive antithrombotic therapy by the end of hospital day two by TBD (5) Increase rate of ischemic stroke patients with LDL>100, or not measured, or were on cholesterol reducing therapy prior to hospitalization who are discharged on statin medication by TBD (6) Increase rate of ischemic and hemorrhagic stroke patients and or caregivers who are given education re: stroke risk, warning signs, and followup by TBD (7) Increase rate of ischemic and hemorrhagic stroke patients who were assessed for rehabilitation by TBD (8) Share data with SNI (9) Report the seven process measures and stroke mortality rate results to the state Y4: Same as Y3 with adjusted rates Y5: Same as Y4 with adjusted rates