Sherwood Park Kings Athletic Club Athlete Medical History Form
advertisement

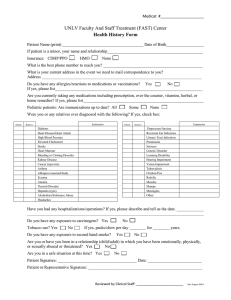
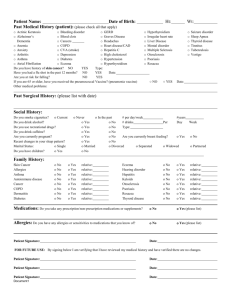
Sherwood Park Kings Athletic Club Athlete Medical History Form First Name __________________________ Last Name __________________________ Date of Birth (DD/MM/YYYY)_____________________ Health Care # _________________________ Province ___________ Home Phone # _________________________ Address___________________________________________________________________ Emergency Contact Information Name _______________________________ Relationship _________________________ Phone # ______________________________ City ________________________________ Family Doctor _________________________ Dr. Phone # __________________________ Medical History – you or anyone in your immediate family Alcohol habit YES NO Intestinal disorder Anemia YES NO Jaundice Appendicitis YES NO Kidney disease Asthma YES NO Bloody urine Blood disorder YES NO Malfunctioning organs Cancer YES NO Missing organs Cyst, tumor or growth YES NO Memory loss Calcium deposits YES NO Motion sickness Chest pain or pressure YES NO Mononucleosis Childhood disease (measles) YES NO Neurological disorder Collapsed lung YES NO Pneumonia Coughed up blood YES NO Recurrent headaches Diabetes YES NO Recurrent nose bleeds Dizziness or fainting YES NO Rheumatic fever Epilepsy YES NO Sexually transmitted disease Excessive bleeding YES NO Shortness of breath Gout YES NO Sinusitis Ear pain YES NO Sickle cell anemia Hearing problems YES NO Skin rash, infection, hives Hearing aid YES NO Severe dental or gum issue Heart disease YES NO Smoking habit Heart murmur YES NO Stomach ulcer Irregular heartbeat YES NO Stroke Heat stroke/exhaustion YES NO Sudden death before 50 Hernia YES NO Surgery/hospitalization Hepatitis YES NO Tonsillitis YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO High or low blood pressure High blood cholesterol YES YES NO NO YES YES NO NO Tuberculosis Vision problem Medical History: Please provide a brief explanation for any of the above YES answers. _____________________________________________________________________________________ _____________________________________________________________________________________ Allergies: List any allergies you have and describe your reaction. _____________________________________________________________________________________ _____________________________________________________________________________________ Medications: List any prescription or non-prescription medications, vitamins or supplements. _____________________________________________________________________________________ _____________________________________________________________________________________ Physical Examination: Date of last physical exam by a medical doctor and results/findings. _____________________________________________________________________________________ _____________________________________________________________________________________ Do you wear glasses or contacts for sports? Wear false teeth, braces, plate or dental appliances? Have you ever been advised not to participate in sports? Do you have any surgical pins, screws or plates in your body? Have you been advised to have surgery but it has not occurred? YES YES YES YES YES NO NO NO NO NO Head Injury History: List any previous head injuries (concussions), date and severity. _____________________________________________________________________________________ _____________________________________________________________________________________ Musculoskeletal Injury History: List any musculoskeletal injuries and if they are still a problem. _____________________________________________________________________________________ _____________________________________________________________________________________ Additional Information: including other medical concerns the trainer should be aware of. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________