6) Write short notes on negative compensation errors? Describe 2
advertisement
 Write short notes on negative compensation errors? Describe 2")
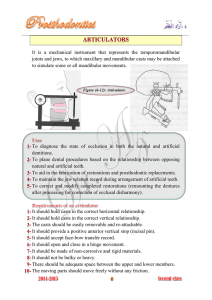
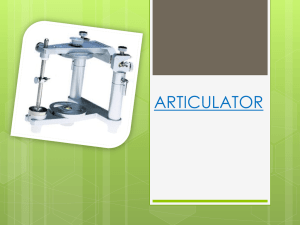
6) Write short notes on negative compensation errors? Describe 2 instances. Negative compensation errors are one which occurs when the articulator over compensates for mandibular movement. This would result in a negative feature such as a groove or fossa that is wider than ideal or conversely a positive feature such as a ridge or cusp that is somehow narrower than ideal. This allows posterior teeth to disclude more freely when the mandible moves. However, when there is good quality CO contact, negative errors are acceptable though excessive negative error can result in a loss of occlusal efficiency and MI stability. Factors that can contribute to negative compensation errors include 1. 2. 3. 4. 5. Condylar guidance Anterior guidance Plane of occlusion Curve of Spee Lateral translational movements For instance: 1. Condylar guidance: a. Angle of condylar inclination set less steep on purpose so to prevent interferences later on especially in protrusive movements b. An excessively steep condylar guidance angle would serve to ‘block’ movements of the mandible c. Results in gentler shorter cusp slopes (corwns, bridges are built with gentler slopes to prevent interferences – ie. Immediate disclution during eccentric movement 2. Lateral translational movement a. Immediate side shift (ISS) is defined as the bodily side shift of the mandible that occurs early, before condyle begins to translate from the fossa b. Determined by morphology of the medial wall of the mandibular fossa, inner horizontal portion of the TM ligament which attaches to the lateral pole of the rotating condyle c. If TM ligament of the rotating condyle is very tight and medial wall is very close to orbiting condyle, then purely rotary movement made around the axis of rotation in the working side condyle (nolateral movement d. Greater ISS generally would lead to gentler shorter cusp slopes 5) Concept of Mutual Protection Theory and rationale of the theory Mutual Protection: A selective pattern of disclusion of non-working tooth surfaces during similar mandibular excursions. In a sense by serving to disclude the non-working side teeth during lateral excursion and posterior teeth during protrusive incisal contact, the working teeth or inclines protect the non-working teeth or inclines. This is because, laterotrusion causes the posterior teeth to contact, however as it is very near the fulcrum(the TMJ as the mandible can be regarded as a class 3 lever) and this creates too much stress on the teeth. Hence, the contacts should be farthest away from the fulcrum, ideally on the anterior teeth. For protrusive movements, even if horizontal forces are acted upon the anteriors, it is still acceptable as the distance from the fulcrum is large and minimal forces are applied to the anterior teeth. Furthermore, the inclined overlapping occluding surfaces of the anterior teeth do not readily withstand vertical loads but are ideally suited to distributing lateral loads. Only involve specialised groups of teeth as in certain centric/eccentric positions of the mandible, certain groups are best able to withstand the occlusal loads and protect other groups from unfavourable forces. In protrusion, the OB-OJ relations of the incisors produce an incisal guidance(anterior guidance) that is steep enough to cause disclusion of all posterior teeth. In lateral excursion, the OB-OJ relationships of the contacting teeth(canine guidance and group function) on the working side should be sufficiently steep to cause disclusion of all non-working teeth. The choice between canine disclusion, partial group function or complete group function depends on clinical factors as - pre-existing tooth relationships - Crown-root ratio -mobility or fremitus Hence in conclusion, anterior teeth, unlike posterior teeth are in proper position to accept the forces of eccentric mandibular movements. Generally, it may be stated that posterior teeth fucntion most effectively in stopping the mandible during closure whereas anterior teeth function most effectively in guiding the mandible during eccentric movements. With appreciation of these roles it becomes apparent that posterior teeth should contact slightly more heavily than anterior teeth in CR. This condition is described as mutually protected occlusion. Write short notes on a) Envelope of madibular incisor b) WS condyle c) NWS condyle a) Envelope of function is defined as the individual jaw movement cycle starting from MI and returning to MI in function. It is a 3-D movement and a masticatory sequence in a composite of several individual envelopes of function (chewing strokes) from the beginning of mastication until deglutition. Madibular movements – Sagittal Plane Posselt’s Envelope 1. Posterior opening border (joint morphology and ligaments) 2. Anterior opening border (joint morphology and ligaments) 3. Superior contact border (occlusal and incisal surfaces) 4. Functional (conditional responses of neuromuscular system) Posterior Opening Border Movement 2 stage hinging movement Stage 1 Stage 2 1. Posterior Opening Border Movements Stage 1 -condyles stabilized in most superior position in the articular fossae -centric relation (CR) position -pure rotation with no translation of condyles 1. Posterior Opening Border Movement Stage 2 -after 20 - 25mm interincisal opening -TM ligaments cause anterior and inferior translation -axis of rotation shifts to rami - sphenomandibular ligament attachments -anterior mandible moves posteriorly and inferiorly -maximum opening : 40 - 60mm interincisal opening -capsular ligaments limit opening 2. Anterior Opening Border Movement -from maximally open to maximally protruded -not a pure hinge movement - posterior movement of condyles from tightening of stylomandibular ligaments 3. Superior Contact Border Movement - totally tooth determined - tooth contact present throughout - Determinants: (1) CR to MI shift (2) posterior cusp steepness (3) vertical and horizontal overlap (4) lingual morphology of maxillary anteriors (5) interarch relationship -CR-MI shift = 90% of population average = 1.25 + 1mm -mesial incline maxillary teeth vs distal inclines mandibular teeth -muscle force applied - superoanterior shift to MI (ICP) -CR-MI shift vertical component lateral component -if CR = MI, no superior slide -from MI, anteriors in contact and slide into anterior guidance - mandibular incisors slide along maxillary lingual fossae -anteroinferior movement (edge to edge and maximum protrusion) 4. Functional Movements -within borders (intra-border movements) -typically begin at and below MI -Chewing stroke in sagittal plane -Postural Position (Clinical Rest Position) -2-4mm inferior to MI -variable Mandibular Movements - Horizontal Plane -Trace with a Gothic arch tracer - rhomboid-shaped pattern Movement Components 1. Left lateral border 2. Continued left lateral border with protrusion 3. Right lateral border 4. Continued right lateral border with protrusion 5. Functional 1. Left Lateral Border Movements -Left condyle - Working (or Rotating) - stays in CR -Right condyle - Nonworking (or Orbiting) - anterior, medial and inferior from right inferior lateral pterygoid pull 2. Continued Left Lateral Border Movements with Protrusion -right condyle at maximum anterior position -contraction of left inferior lateral pterygoid -mandibular midline shifted back to facial midline 3. Right Lateral Border Movements -Right condyle - Working (or Rotating) - stays in CR -Left condyle - Nonworking (or Orbiting) - anterior, medial and inferior from left inferior lateral pterygoid pull 4. Continued right lateral border with protrusion -Left condyle at max anterior position -Contraction of Right inferior lateral pterygoid -Mandibular midline shifted back to facial midline 5. Functional Early stage of mastication Late stage of mastication -moves closer to MI Mandibular Movements - Frontal Plane -not traditionally traced Movement components 1. Left lateral superior border 2. Left lateral opening border 3. Right lateral superior border 4. Right lateral opening border 5. Functional 1. Left Lateral Superior Border Movements -Inferior concave path -Primary determinant - interarch relationships and morphology -Secondary determinant - condyle-disc-fossa relationship - working side TMJ morphology -Maximum extent: determined by ligaments of working side joint 2. Left Lateral Opening Border Movements -max opening produces a laterally convex path -ligaments cause a shift back to midline as maximum opening is approached 3. Right Lateral Superior Border Movements -Inferior concave path -Primary - interarch relationships and morphology -Secondary - condyle-disc-fossa relationship - working side TMJ morphology -Maximum extent : ligaments of working side joint -May be different from 1 due to unequal tooth contact 4. Right Lateral Opening Border Movements -laterally convex similar to Left Opening Movement -ligaments cause a shift back to mandibular midline as maximum opening is approached 5. Functional Movements -drops down -opening determined by bolus size -shifts to side of bolus -rises up through bolus -shifts back to MI Envelopes of Motion -3 planes : 1. sagittal 2. horizontal 3. frontal Conclusion: By combining the mandibular border movements in the 3 planes, a 3D envelope of motion can be produced that represents the maximum range of motions of the mandible. Although the envelope has its characteristic shape, differences will be found from person to person. Generally, the superior border of the envelope is determined by tooth contacts whereas the other borders are primarily determined by ligaments and joint anatomy that restrict or limit movements. (b) + (c) 1. Mandibular movement is a complex series of interrelated 3D rotational and translational actions. It is defined by the combined and simultaneous action of both TMJ 2. Although they cannot function independently, they seldom function in identical motions 3. Rotation occurs in the working side condyle, in other words, the teeth can be separated and then occluded with no positional change in this condyle 4. This rotation takes place in the inferior joint cavity and can occur in 3 axes, the vertical horizontal and sagittal axis. 5. The working condyles rotates on what is known as the terminal hinge axis and is the condyle that does not translate during lateral motion 6. The non-working side condyle is on the non functional side and orbits instead of rotating 7. Rotation of the mandible about a vertical axis through the working side condyle occurs when the non-working side condyle translates anteriorly, inferiorly and medially down its associated articular eminences. Thus the mandible is said to make a lateral excursion to the working side. 8. In canine guidance or group function there should be no tooth contact on the non-working side. If there is contact, this is referred to as non-working interference. Articulators Non-adjustable Articulator Simplest type of articulator as no adjustments are possible to adapt it more closely to the specific condylar movements of the patient Many of these articulators allow for eccentric movement however only average values and accurate duplication of eccentric movement for a specific patient is impossible. Even opening and closing pathways of the teeth do not replicate that of the patient Only one accurate and reproducible position can be used and that is inter-cuspal position Advantages: o Relatively inexpensive o Small amount of time invested in mounting procedure of casts Disadvantages: o As articulator only produces one contact point, a restoration cannot be properly prepared to meet the occlusal requirements of the eccentric movements of the patient. Hence more time would be allocated to intraoral adjustments of restorations which will affect final occlusal relationship and anatomical features of restoration. Semi-adjustable Articulator Permits more variability than the non-adjustable articulator and has 3 different adjustments to closely duplicate the condyle movements of the patient. Hence, an occlusal contact position can be accurately duplicated which also allows for the duplication of eccentric movements as well. Adjustments on the semi-adjustable include o Condylar inclination o Lateral translational movement(ie Bennet’s angle) o Intercondylar distance Condylar inclination represents the angle at which the condyle descends along the articular eminences in the sagittal plane Bennet’s Angle is the angle described by the inward movement of the condyle during laterotrusive movement Intercondylar distance is the distance between the rotational centres of the condyles Advantages o Adaptability of the articulator to the patient’s specific condylar movements allows for restorations that more closely fit the occlusal requirements of the patient to be fabricated thus minimizing the need for intraoral adjustments. Disadvantages o Compared to non-adjustable it is much more expensive and more time is needed to collect and transfer information from the patient to the articulator Fully-adjustable Articulator Most sophisticated instrument in dentistry for duplicating mandibular movements Has four different adjustments to accurately repeating the condylar movements seen in the patient o Condylar inclination o Bennet’s angle or ISS o Rotating condylar movement o Intercondylar distance Adjusting the rotating condylar movement is not available in the fully adjustable articulator(the other adjustments are). During laterotrusive movement, the rotating, or working side condyle does not purely rotate around a fixed point but also moves slightly laterally. This lateral shift can be superior, inferior, forward or backwards. Advantages: o Ability to accurately duplicate mandibular movement, hence intraoral adjustments of restorations are usually minimal Disadvantages: o Expensive o A lot of time required to transfer information properly from patient to the articulator Selection Of Articulator: 1. Characteristics of patient’s occlusion Two factors determine the mandibular movement, mainly anterior tooth guidance and posterior condylar guidance One of the more important functions of the articulator is to provide influence on the posterior determinants a less sophisticated articulator can be used for patients with adequate and immediate anterior guidance and these tooth generally dominate in controlling mandibular guidance 2. Extent of Restorative procedures Primary need for articulator is to minimize the amount of time spent on intra oral adjustments Chair time required to programme a fully adjustable articulator often makes it impractical for the fabrication of a single crown Generally more extensive treatments require more sophisticated articulator systems and minor procedures can be done with simpler instruments 3. Understanding the limitations of the articulator system The advantages and disadvantages of each articulator system must be understood if the proper instrument is to be selected 4. Skills of technician An articulator only as accurate as the clinician who uses it A semi-adjustable articulator in the hands of a knowledgeable clinician may be of greater assistance in treatment than a fully adjustable articulator in the hands of an inexperienced operator