Pressure Ulcer Prevention Gap Analysis Tool

Pressure Ulcer (PULC)
Prevention Strategies and Gap Analysis
Gap Analysis Questions
Yes
All
Units
Yes
Some
Units
Just
Starting
If answered question “NO” – or just starting indicate the priority, person responsible and target and implementation date.
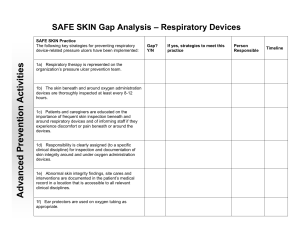
Respiratory Devices
1a) Respiratory therapy is an active member of the pressure ulcer prevention team.
1b) A respiratory therapy champion(s) is designated for pressure ulcer prevention related to respiratory devices.
1c) The respiratory therapy champion(s) partners with the skin champion(s) to provide education and protocols for respiratory therapists and nursing staff on the proper fitting of CPAP/BiPAP masks.
1d) The respiratory therapy and safe skin champion(s) partner to provide coaching to respiratory therapy staff and nursing staff related to skin inspection and pressure ulcer prevention practices related to respiratory devices.
1f) Respiratory therapy is included in root cause analyses in cases involving respiratory device-related pressure ulcers.
1g) Soft flexible tubing (i.e., silicone tubing) is the standard oxygen tubing used hospital-wide.
1h) If a soft oxygen tubing option does not exist (i.e., high-flow oxygen tubing), ear protectors are used to protect skin around the ears.
1i) Patients and families are educated on how they can help prevent pressure ulcers from respiratory devices.
1j) The organization requires, and assigns responsibility for, the inspection of skin beneath and around oxygen administration devices each shift and during respiratory therapy treatments and oral cares.
1k) The organization has protocols and processes in place for protecting the skin when patients are placed in a prone position.
1l) Strap tension and skin integrity beneath and around life sustaining
Bi-PAP and NPPV masks are checked at least every 4 hours, with oral intake, and with oral cares.
1m) During routine tracheostomy site care (at least every 8-12 hours), skin integrity and tension is checked under the straps, around and in back of the neck, around the stoma, and under the tracheostomy tube flange/faceplate.
1n) The tension and skin integrity under and around ETTs and straps is checked every 2 hours, when repositioning patient, with close attention to the neck, lips and mouth.
Acknowledgement: Adapted from Minnesota
Hospital Assocation Patient Safety Road Map, used with permission
1o) For neonates (age <28 days from expected due date), the tension and skin integrity under and around ETTs and straps is checked during routine cares, with close attention to the neck, lips and mouth.
1p) When using commercial stabilizers (commercial stabilizers are preferred), the position of the ETT is rotated at least every 2 hours when repositioning patient in the direction the patient is positioned (i.e., if patient is positioned on left side, rotate ETT to the left; when patient is repositioned to right side, rotate ETT to the right).
1q) An order set, protocol, or documented process is in place for the management of newly placed tracheostomy tubes, including suture removal, following surgery to reduce the potential for pressure ulcers developing in and around the faceplate and flange.
1r) Starting post-op day 5, a trigger is in place for daily re-evaluation of the need for sutures to secure a newly placed trach.
Hospital Specific Strategies:
Coccyx/Sacrum Pressure Ulcers
2a) A re-positioning schedule is developed and followed for each patient based on the patient’s condition (maximum time between turns = 2 hours). The repositioning schedule takes into account time spent in supine positions during meals, visits, sitting, OR, procedures, etc.
Additional supine positioning may not be indicated.
2b) Interdepartmental approaches are implemented to keep patients in positions other than supine throughout their stay, e.g., therapy places patient in position other than supine when returning from therapy, radiology staff positions patient in position other than supine after procedures (if appropriate), repositioning schedule reduces number of times patient is in supine position, bed is moved so patient can see the television when not in supine position, patient is placed in position other than supine following ambulance transport, patient is encouraged to eat meals out of bed if able.
Hospital Specific Strategies:
Staff involved with patient handling receives training on how to effectively reposition patients to redistribute pressure, including staff in the following roles:
2c) Nurses
2d) Nursing assistants
2e) Radiology
2f) Therapy
2g) Transport
2h) A process is in place for patients to be repositioned during dialysis.
2i) Adherence with repositioning is visually monitored by unit leadership and/or skin champion(s) and coaching provided when gaps are identified.
2j) Staff receive coaching on how to engage patients and families in the importance of repositioning.
Acknowledgement: Adapted from Minnesota
Hospital Assocation Patient Safety Road Map, used with permission
2k) There is an escalation process in place for patient refusal to reposition (i.e., informed refusal algorithm).
2l) Nursing staff receive education for repositioning hemodynamically unstable patients.
Hospital Specific Strategies:
If a patient is not able, or it is anticipated that they will not be able, to be adequately or routinely repositioned:
2m) An immediate and on-going evaluation is performed for an advanced support surface with features and components such as low air loss, viscous fluid, air fluids, or alternating pressure.
2n) An advanced support surface is readily available so that patients with anticipated medical contraindications to repositioning can be initially placed on an appropriate surface.
2o) If there is a perceived barrier to optimal repositioning of a patient (i.e., patient may be too unstable to turn; patient may not be able to be positioned on a particular side), there is a process in place for an inter- professional discussion with the healthcare team to determine if the patient is not able to be optimally repositioned and to develop a plan for off-loading pressure (i.e., slow incremental turns vs. 30 degree turns).
2p) At least hourly micro-turns (slow incremental turns; 10-15 degrees) off pressure points, especially the tailbone and occiput, are implemented until optimal repositioning is resumed.
2q) If a patient is on an alternate repositioning plan, retrials are conducted every 8 hours to re-evaluate for optimal (30 degree every
2 hours) repositioning.
2r) A repositioning schedule is developed for patient’s post-surgery to ensure patient does not remain on their back (or in surgical position) for extended periods of time. If possible, patient’s first position, postsurgery, should be in a different position than their position during surgery and in the PACU.
2s) As a high risk factor for pressure ulcers, there is a process is in place to monitor (e.g., collect during P&I studies) and reduce incontinence associated dermatitis (IAD) or diaper dermatitis.
2t) Support surfaces are evaluated across the organization for appropriate pressure redistribution properties (e.g. OR beds, chair cushions, transport carts, radiology tables, emergency department gurneys).
2u) A plan/process is in place for replacement or supplementation of surfaces that do not provide adequate pressure redistribution for patients at risk.
2v) When a patient is in a supine position, the head of the bed (HOB) is kept at 30 degrees or less (unless medically contraindicated) to prevent pressure, friction, and shear. If HOB 30 degrees or less is medically contraindicated, patient is placed on a higher specification support surface.
Hospital Specific Strategies:
Documentation
Acknowledgement: Adapted from Minnesota
Hospital Assocation Patient Safety Road Map, used with permission