R_-_Complement
advertisement

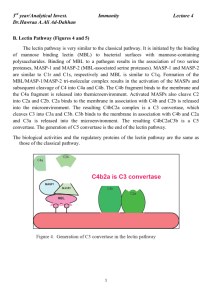
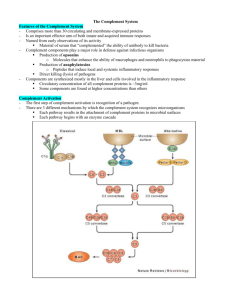
Complement (Regal) (1) (2) (3) (4) (5) (6) Circulating plasma proteins with membrane bound regulators. This is a primitive microbial scanning system that acts independent of T cells and antibodies (Innate). It is a major effector system for humoral immunity (Acquired). Heat labile. Made by liver hepatocytes & by tissue macrophages, but also in epithelial cells, fibroblasts & monocytes. The sequence is: C1-C4-C2-C3-C5-C6-C7-C8-C9 Specific functions include: lysis, opsonization of Ag Mediation of the inflammatory response *Solubilization of immune complexes (helps the Ag: Ab complex be eliminated) *Augment stimulation of the B cell Three specific pathways exist: classical, mannose-binding lectin, and alternative C3a/C5a are mediators of inflammation C3b functions as an opsonin and to amplify adaptive immunity C5-C9 forms the membrane attack complex Classical pathway or C3 deficiencies are associated with immune-complex disease and pyogenic (pus forming) infections. Alternative pathway deficiencies can also results in pyogenic infections. MBL pathway deficiency can results in serious pyogenic infections in neonates and children. Membrane attack complex deficiencies are associated with Neisseria infections Complement is good for immune-complex clearing and fighting infections and killing bacteria. Plasma concentrations are the greatest for C3 (1.2mg/ml) Complement Activation (1) (2) (3) (4) Activating factors include Ag:Ab complexes, microbial polysaccharides, and LPS/foreign surfaces (glass)/nucleophiles for the classical, MBL, and alternative pathways, respectively The classical pathway must have had a specific immune response already before activation; while the MBL and alternative pathways deal with innate immunity and pattern recognition. Proteolytic cleavage of complement components occurs through C5 Non-proteolytic cleavage occurs in the terminal lytic pathway (no enzymes) Classical Pathway Activation (142356789) (1) (2) (3) (4) (5) C3 convertase is the product desired from the classical pathway, which cleaves C3C3b/C3a Triggered by antigen binding two IgG’s (Ag:2IgG)or one IgM (Ag:IgM) Cascade of proteolytic steps performed by serine esterases. Covalent attachment of C4b and C3b to bacterial surface via thioester bonds tags it for destruction!!! C1 is present in the plasma as inactive C1qr2s2 complex, subsequent binding of 2 IgG or 1 IgM induces conformational change in C1q, leading to a cascade in changes and finally C4 cleavage (6) (7) (8) (9) (10) (11) (12) Activated C1qr2s2 = C1 esterase cleavage of C4, controlled by C1 inhibitor (C1INH); C1INH absence gives rise to hereditary angioedema. C4 can act as an opsonin if nothing else happens. 1000X more IgG than mIgM is required for activation of C1q due to proximity. C1 esterase cleaves C4 C4b binds to the membrane (thioester bond), nearby C2 is then cleaved by C4b C4b2a (on surface) = C3 convertase (classical pathway) Subsequently, passing C3 gets cleaved by C4b2a and C3b binds the membrane (thioester bond) C4b2a3b = C5 convertase The end result is to amplify and permanently tag the bacterium via covalent attachment ; 1 C1 leading to 10000 C3b’s Mannose Binding Lectin Pathway (1) (2) (3) (4) No specific Ab required. MBL ~ C1q with MBL binding to bacterial surface mannose and C1q binding to IgG. MASP-1/2 ~ C1r2s2 cleaves C4 Leads to C1 independent formation of the classical pathway C3 convertase (C4b2a) Alternative Pathway (promiscuous) (1) (2) (3) (4) (5) (6) (7) No specific Ab needed. Spontaneous hydrolysis of C3 (1%) allows Factor B to bind C3(H2O) or C3b FB-C3b or FB-C3(H2O) then binds Factor D, which cleaves FB, resulting in the formation of C3bBb (C3 convertase) Properdin stabilizes the alternative pathway C3 convertase (C3bBb) – allowing enzyme to last longer. C3 is deposited continuously and randomly on surfaces, continuation of the pathway depends on other surface features Surfaces rich in carbohydrate and deficient in sialic acid are the best activators C5 convertase – C3bBbC3b (CP C4b2a3b) Terminal Complement Pathway (1) (2) (3) C5 is cleaved by either the AP or CP C5 convertase C3bBbC3b and C4b2a3b, respectively 2 fragments C5b interacts with C6-C9 to form the membrane attack complex (transmembrane channel allowing passage of ions and lysis of cell) via conformational changes, not enzymatic reactions. Lysis can occur in the absence of C9, but is slower Regulation of Complement (1) Factor H is a fluid phase inhibitor of Alternative Pathway C3 convertase; thus, if C3bBb is floating around, Factor H binds to it and dissociates Bb, leading to a decay acceleration of the convertase. (2) If Factor H sees C3bBb on a membrane with sialic acid (like our own), it can bind sialic acid and C3b, displacing Bb from the convertase and inactivating C3bBb. Factor I will then degrade C3b w/ Factor H as cofactor. (3) Activator surface (like bacteria) don’t have sialic acid no Factor H binding, no displacement of Bb C3 convertase not inhibited, which is good b/c then it will die. Complement deficiency (1) (2) C1 inhibitor deficiency causes hereditary angioedema due to loss of C1 esterase (C1qr2s2) inhibition. Episodic edema sx, lots of fluid leakage into extravascular space. Also inhibits kallikrein, plasmin, Factor Xia & Factor XIIa which are clotting factors. DAF (CD55) & CD59 deficiency increases RBC MAC-mediated lysis susceptibility; treatment with anti-C5 antibody may reduce hemolysis but increase Neisseria infection. If C3b or C4b are attached to the surface they can do one of 3 things: 1) pathway proceeds MAC is made Cell lysis occurs. 2) Interact w/ CR1 opsonization & clearance of IC 3) If C3b degrades faster than the pathway can keep up with C3bi, C3dg, C3d are made on surface that will interact w/ complement receptors RBCs &WBCs have tons of CR1 while B cells have CR2 (augments humoral immunity via making more Ab) CR1 on RBCs is involved in the transport of immune complexes to the liver and also blocks C3 convertase formation; thus C3b and C4b interact with CR1 on RBCs and are delivered to the liver for elimination. Complement receptors: o CR1 (CD35) – major ligands are C3b & C4b, monocytes, MOS, PMN, eosinophil, RBC, B & T cells, promotes binding of opsonized microbes to RBCs, helps in transport of immune complexes by RBCs, promotes phagocytosis in cooperation w/ Fc receptors , blocks formation of C3 convertase, No lysis. o CR2 (CD21) – major ligands are C3d, C3dg, iC3b, B cells, activated T cells & epithelial cells, forms an additional signal to help stimulate the B cell to increase the humoral response, has high affinity for an envelope protein of an Epstein barr virus, allowing the virus to enter the B cell. o CR3 & CR4 – major ligand iC3b, monocytes, macrophages, PMN, NK cells, T cells, phagocytosis, cell adhesion REMEMBER: C3 is cleaved by both the alternative pathway and classical pathway C3 convertase. C3b & C4b covalently attach to the activator surface. C3a & C5a are anaphylatoxins, WBCs will accumulate b/c these are chemotactic, MIMIC the sx of inflammation & anaphylaxis! also, smooth muscle contraction, increased vascular permeability, degranulation of mast cells. C5a receptor is CD88. They each have their own kind of receptor. Review: Biological effects of complement activation: Host defense: Lysis (MAC), Opsonization (C3b & C4b & their degradation products are opsonins), Viral neutralization (lysis, opsonization or interference w/ viral attachment to host cells) Augments humoral immunity via the CR2 receptor (CD21) Pro-inflammatory effects (C3a, C5a) Solubilization & Clearance of Immune Complexes o Depositing insoluble aggregates in the tissues can cause damage & IC disease. Binding of C3b to the Ag:Ab complex interferes w/ lattice formation, limits its growth, prevents precipitation of the Ag:Ab complexes and keeps them soluble. o Immune complexes coated w/ C3b bind to CR1. CR1 receptors on RBC are responsible for the transport of the immune complexes to the RES system for clearance (macrophages in spleen, etc). The immune complex coated w/ C3b is transferred from the RBC CR1 receptor to the MOS CR1 receptor. Immune complex is then internalized & degraded. Immune complex diseases: High incidence of IC disease in ppls that are deficient in C1, C4, C2, C3 b/c immune complexes aren’t solubilized & cleared Complement can also play a significant role in tissue damage in IC disease like SLE (systemic lupus erthematosus) o Excess immune complexes cause pathological complement activation inflammation, tissue damage