File
advertisement

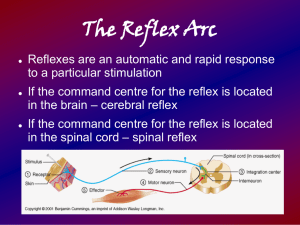
Tiphaine Gilbert DCR TUTORIAL 5 - NEUROLOGICAL EXAM (MOTOR) HISTORY – What in the history points to the need for a Motor exam? Weakness, fall, dropping, tripping, fasciculation, involuntary movements. OBSERVATION – Starts with your first sight/touch of the patient, how do they move breathe, stand, talk etc. What aspects of their stance or gait might suggest neuro-motor deficits? Hemiballismus (violent movement), dystonia (contraction of antagonist), tics, dyskinesia (tics in face), tremor (rhythmic movement), involuntary movement, myoclonus (mm jurks), chorea, bradykinesia (slow movement). TONUS & CLONUS – What is the definition of Tonus? How is it tested? Tonus: A state of partial contraction present in a muscle in its passive state (UMNL). Test: Roll arms and legs, slide heals on the table. What types of Hypertonia do you know? What about Hypotonia? What might these imply? Hypertonia: Abnormal increase in muscle tension and a reduced ability of a muscle to stretch (UMNL). Hypotonia: State of low muscle tone (the amount of tension or resistance to movement in a muscle), often involving reduced muscle strength. What is Clonus, how might you elicit it, what is implied by its presence? Clonus: Series of involuntary, rhythmic, muscular contractions and relaxations. Clonus is a sign of certain neurological conditions, particularly associated with upper motor neuron lesions involving descending motor pathways, and in many cases is, accompanied by spasticity (another form of hyperexcitability). Test: Clonus at the ankle is tested by rapidly flexing the foot into dorsiflexion (upward), inducing a stretch to the gastrocnemius muscle. Subsequent beating of the foot will result, however only a sustained clonus Tiphaine Gilbert (5 beats or more) is considered abnormal. Clonus can also be tested in the knees by rapidly pushing the patella (knee cap), towards the toes and the wrist by holding on extention and forcing extension. What is Hemiplegia ? Paraplegia? Quadraplegia? Hemiplegia: Total paralysis of the arm, leg, and trunk on the same side of the body. Paraplegia: Impairment in motor or sensory function of the lower extremities. Quadraplegia: Paralysis of all four limbs. Also called tetraplegia. Tiphaine Gilbert DEEP TENDON REFLEXES – How are these elicited? What responses might be found and what is implied by them? What nerve root levels are being tested in each reflex? Testing the reflexes assesses the integrity of the reflex arc and the supraspinal influence that affect it. Mm Level Nerve Biceps C5/6 Musculocutaneous nerve Brachioradialis C5/6 Radial nerve Supinator C5/6 Pronator C6/7 Median nerve Action Normal response Elbow flexion Elbow flexion and forarm supination Hold the patient’s Pronation of hand vertically so the the forearm wrist is suspended. From the medial side, strike the distal end of the radius directly with a horizontal blow. Tiphaine Gilbert Triceps C6/7 or C7/8 Radial nerve Fingers jerk Knee Quadriceps reflex C8 L2/3/4 Femoral nerve Adductor reflex L2/4 Obturator nerve Hamstring reflex L4/S2 Sciatic nerve Ankle Achilles reflex L5/S2 Tibial nerve Elbow extension Knee extension At medial epicondyle of femur, adductor magnus att Hip and knee flexed at about 90 degrees and slight ext. rot. Tap on medial hamstring tendon Thigh adduction Flexion of knee and contraction of medial mass of hamstrings Contraction of gastrocnemius and plantarflexion of the foot. Tiphaine Gilbert What do you understand by the “Reflex Arc”? What element in the muscle actually implements the reflex? Is the Golgi Tendon Organ involved? What is an “Inverted Reflex”, and what might it indicate. Reflex arc: Neural pathway that controls an action reflex. Most sensory neurons do not pass directly into the brain, but synapse in the spinal cord. This characteristic allows reflex actions to occur relatively quickly by activating spinal motor neurons without the delay of routing signals through the brain, although the brain will receive sensory input while the reflex action occurs. There are two types of reflex arc: autonomic reflex arc (affecting inner organs) and somatic reflex arc (affecting muscles). (Efferent neuron = LMN) Absent stretch reflexes= lesion in the reflex arc itself. Associated symptoms and signs usually make localization possible: 1. Absent reflexes and sensory loss in the distribution of the nerve supplying the reflex: the lesion involves the afferent arc of the reflex—either nerve or dorsal horn. 2. Absent reflex with paralysis, muscle atrophy, and fasciculations: the lesion involves the efferent arc—anterior horn cells or efferent nerve, or both. Most common: Peripheral neuropathy. Muscle diseases do not produce a disturbance of the stretch reflex unless the muscle is rendered too weak to contract. This occasionally occurs in diseases such as polymyositis and muscular dystrophy. Tiphaine Gilbert Hyperactive stretch reflexes are seen when there is interruption of the cortical supply to the lower motor neuron, an "upper motor neuron lesion." The interruption can be anywhere above the segment of the reflex arc. Analysis of associated findings enables localization of the lesion. The stretch reflexes can provide excellent clues to the level of lesions along the neuraxis. For example, if the biceps and brachioradialis reflexes are normal, the triceps absent, and all lower reflexes (finger jerk, knee jerk, ankle jerk) hyperactive, the lesion would be located at the C6–C7 level, the level of the triceps reflex. The reflex arcs above (biceps, brachioradialis, jaw jerk) are functioning normally, while the lower reflexes give evidence of absence of upper motor neuron innervation. Segmental Innervation of Stretch Reflexes. The laterality of reflexes is also helpful. For example, if all the reflexes on the left side of the body are hyperactive and those on the right side are normal, then a lesion is interrupting the corticospinal pathways to that side somewhere above the level of the highest reflex that is hyperactive. Individual nerve and root lesions can be identified by using information about the reflexes along with sensory and motor findings. The reflex arc is broken if any one of its elements malfunctions. The physical sign of an interrupted reflex arc is a diminished or absent reflex. When the descending motor pathway (the pyramidal tract) in the spinal cord is injured above the level of the reflex arc, normal cortical inhibition is lost, producing a hyperactive or spastic reflex. 0, 0 1, + 2, + + 3, + + + 4, + + + + No response Detectable only with reenforcement Easily detectable Brisk with at most a few beats of clonus Sustained clonus Tiphaine Gilbert SUPERFICIAL REFLEXES – What superficial reflexes do you know? How are they tested. What responses might you get and what do they mean? Receptors organs in the skin rather than in mm fibers. Lost in disease of the pyramidal tract. Abdominal reflex (T5/12): Reflex stimulated by the stroking of the abdomen around the umbilicus that results in contraction of the abdominal muscles; typically the umbilicus moves towards the source of the stimulation. The afferent is cutaneous sensory (tickle and light touch) that is dermatomal and the efferent limb is the segmental innervation of the abdominal muscles. The reflex is typically lost in upper motor neurone syndromes. This reflex is also lost due to a variety of causes, including age, abdominal surgery, obesity, pregnancy and in parous woman. Plantar response (L4/S2): Reflex elicited when the sole of the foot is stimulated with a blunt instrument. The reflex can take one of two forms. In normal adults the plantar reflex causes a downward response of the hallux (flexion). An upward response (extension) of the hallux is known as Babinski response. The presence of the Babinski sign can identify disease of the spinal cord and brain in adults (Pyramidal lesion), and also exists as a primitive reflex in infants. Tiphaine Gilbert POWER – How do you test power? Do you know the nerve root levels for the muscles you commonly test? What are potential causes of muscle weakness? What is fasciculation and when might it be encountered? Can you state a common “pattern” of weakness and what it implies? Compare signs of Upper and Lower Motor Neurone lesions. C1-2 – Head flexion C2-3- Shoulder shrug C5 – Shoulder extension C6 – Arm flexion - Biceps C7 – Arm extension - Triceps C8 – Wrist extensors T1 – Hand grasp L2 – Hip flexion - Iliopsoas L3 – Knee extension - L4 – Knee flexion - hamstrigs L5 – Ankle dorsiflexon - Tibialis ant. S1 – Ankle plantar flexion - Gastrocs Causes of mm weakness: Muscle weakness is a decrease in muscle strength, and it can be caused by a neurologic, muscular or metabolic disorder. Neurologic disorders causing muscle weakness include amyotrophic lateral sclerosis (ALS, also known as Lou Gehrig’s disease), Guillain-Barre syndrome (an autoimmune nerve disorder), stroke, or even a pinched nerve. Muscular disorders, such as muscular dystrophy and dermatomyositis, are also common causes of muscular weakness. Metabolic conditions that can lead to weakness include Addison’s disease, low sodium or potassium levels, and hyperparathyroidism. Ingestion of toxic substance, such as insecticides, nerve gas, or paralytic shellfish poisoning, can cause muscle or nerve damage along with muscle weakness. Muscle weakness can also result from blood disorders, such as anemia and low blood sugar (hypoglycemia). Grading of muscle strength (oxford scale) Grade 0: No muscle movement Grade 1: Muscle movement without joint motion Grade 2: Moves with gravity eliminated Grade 3: Moves against gravity but not resistance Grade 4: Moves against gravity and light resistance Grade 5: Normal strength Tiphaine Gilbert Fasciculation: Small, local, involuntary muscle contraction and relaxation which may be visible under the skin or detected in deeper areas by EMG testing. They arise as a result of spontaneous depolarization of a lower motor neuron leading to the synchronous contraction of all of the skeletal muscle fibers within a single motor unit. Fasciculations can happen in any skeletal muscle in the body. Fasciculations have a variety of causes, the majority of which are benign, but can also be due to disease of the motor neurons. Fasciculations are commonly encountered in healthy people and are rarely bothersome. In some cases the presence of fasciculations can be annoying and interfere with quality of life. In such cases, where the remainder of the neurological exam is normal, and EMG testing does not indicate any additional pathology a diagnosis of benign fasciculation syndrome is usually made. UMN Spastic paralysis No wasting No fasciculation Brisk reflexes Clonus Extensor palmar response (Babinski) LMN Flaccid paralysis Mm Wasting Fasciculation present Reduced or absent reflexes No clonus Plantar response flexor or absent Tiphaine Gilbert CO-ORDINATION – What area of the brain is mostly involved in coordination? What are commonly used tests for co-ordination? What findings indicate abnormality? What is Ataxia? Why should you test joint position sense before testing co-ordination? What is a pendular reflex and what does it indicate? Cerebellum- Cerebellar dysfunctions Motor coordination is the combination of body movements created with the kinematic (such as spatial direction) and kinetic (force) parameters that result in intended actions. Motor coordination is achieved when subsequent parts of the same movement, or the movements of several limbs or body parts are combined in a manner that is well timed, smooth, and efficient with respect to the intended goal. This involves the integration of proprioceptive information detailing the position and movement of the musculoskeletal system with the neural processes in the brain and spinal cord which control, plan, and relay motor commands. The cerebellum plays a critical role in this neural control of movement and damage to this part of the brain or its connecting structures and pathways results in impairment of coordination, known as ataxia. Pendular reflex: An abnormal response to a stimulus applied to the sensory components of the nervous system. This may take the form of increased, decreased, or absent reflexes. Tests: Alternate heel to knee and heel to toe Alternate nose to finger Heel to shin Tiphaine Gilbert STANCE & GAIT – What type of gait abnormalities can you list? What underlying conditions might be responsible? Describe Romberg’s test? What is being tested? Gait abnormalities Hemiballismus Definitions Very rare movement disorder. Involuntary flinging motions of the extremities. Dystonia Sustained muscle contractions cause twisting and repetitive movements or abnormal postures. Tics A sudden, repetitive, nonrhythmic motor movement or vocalization involving discrete muscle groups. Movement disorder which consists of effects including diminished voluntary movements and the presence of involuntary movements, similar to tics or chorea. rhythmic movement Dyskinesia Tremor Involuntary movement Myoclonus Chorea mm jurks Bradykinesia slow movement Underlying conditions Structural brain lesions but can occur with metabolic abnormalities e.g. strokes, brain injury, neoplasm… May be hereditary or caused by other factors such as birth-related or other physical trauma, infection, poisoning (e.g., lead poisoning) or reaction to pharmaceutical drugs, particularly neuroleptics. ???? Tiphaine Gilbert