Assessment of the Neurological System
advertisement

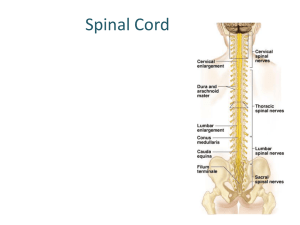
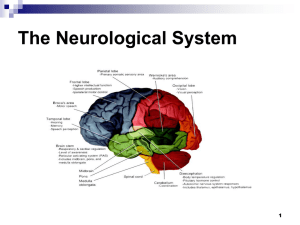
Assessment of the Neurological System Christine M. Wilson Viterbo University Objectives Structure and Function Developmental considerations Neurological assessments Subjective data Objective data Structure and Function Central Nervous System (CNS) Brain and spinal cord Peripheral Nervous System Cranial nerves (12) Spinal nerves (31 pair) All branches of nerves (nerve: bundle of fibers outside of CNS) Central Nervous System Cerebral cortex Cerebrum’s outer layer of nerve cell bodies Controls thought, memory, reasoning, sensation, and voluntary movement Cerebrum-two hemispheres Right and Left Each hemisphere divided into 4 lobes Lobes Frontal Personality, behavior, emotions, intellect Parietal Primary center for sensation Occipital Primary visual receptor center Temporal Primary auditory receptor center Communication areas Wernike’s area in temporal lobe is associated with language comprehension Receptive aphasia Broca area in frontal lobe responsible for motor speech Expressive aphasia Additional CNS ‘parts’ Basal ganglia Deep in cerebral hemispheres Control automatic “associated” body movements Thalamus Relay station; synapses (sites of contact b/tw neurons) for sensory pathways from spinal cord and brain stem to cerebral cortex Cerebellum Operates below conscious level Motor coordination of voluntary movements, equilibrium, muscle tone, posture Brain stem Central core of brain: midbrain, pons, medulla Spinal cord Structure occupying upper 2/3 vertebral canal Ascending/descending fiber tracts between brain and spinal nerves; mediates reflexes Pathways of CNS Crossed representation Left cerebral cortex receives sensory information from and controls motor function to right side of body Right cerebral cortex receives sensory information from and controls motor function to left side of body Sensory Pathways (p.664) Sensory receptors in skin, mucous membranes, muscles, tendons, viscera Sensation travels through peripheral nerve to spinal canal and into spinal cord Spinothalmic tract: pain, temperature, crude and light touch Posterior (dorsal) column: sensations of position, vibration, fine localized touch Motor Pathways (p.665) Corticospinal (pyramidal) tract Motor nerve fibers originating in motor cortex Travel to brain stem, then to spinal cord Mediates voluntary movement; skilled, discrete, purposeful movements Extrapyramidal tracts All motor nerve fibers outside pyramidal tract Controls muscle tone, gross automatic movements Peripheral Nervous System Carries sensory messages to central nervous system (CNS) Carries motor function messages from CNS to muscles and glands Carries autonomic messages to internal organs and blood vessels Reflex Arc (p.666) Basic defense mechanism of nervous system; quick reaction to potential pain/damage Involuntary, below LOC control Helps body maintain balance & muscle tone Tapping tendon stretches muscle spindles which activates sensory nerve Message travels from receptor into spinal canal and synapses with motor neuron Message leaves spinal canal and travels to muscle Developmental Considerations Infants Neurological system not completely developed Motor activity under control of spinal cord and medulla Neurons are not yet myelinated Movement directed by primitive reflexes Sensory-motor development: head to extremity The Aging Adult General atrophy with steady loss of neurons in brain and spinal cord Decrease in weight and volume of brain and nerves General loss of muscle bulk, tone, strength, impaired fine coordination, loss of vibratory sense, loss of Achilles reflex Decreased velocity of nerve conduction Slowing of motor system and movement Decreased cerebral blood flow Neurological assessments Complete—person with neurological concerns/dysfunction Mental status Cranial nerves Motor system Sensory system Reflexes Screening—well persons with no significant subjective findings Tongue blade Tuning fork Cotton wisps Percussion hammer ‘familiar’ items Subjective Data Headaches Head Injury Dizziness, vertigo Seizures Tremors Weakness Incoordination Numbness/tingling Dysphagia Dysphasia Past history Environmental hazards Objective Data Inspect and Palpate Motor system Muscles Size: compare bilaterally; measure if needed Strength: check muscle groups by push/pull Tone: PROME; mild resistance, flaccid, spastic Involuntary movements: location, frequency, amplitude Cerebellar Function: Balance Gait Walk 10-20 ft.; smooth, effortless, alternating arm swing Tandem walk Heel to toe Romberg Test Feet together, arms sides, close eyes; hold position 20 sec.; STAND CLOSE Coordination and Skilled Movements Rapid alternating movements Pat knees with hands, palm to back, alternating Finger to finger Person touches your finger, then his nose, then your finger; move position of your finger; smooth, accurate Finger to nose Close eyes, extend arms, touch tip of nose with index finger, alternating; smooth, accurate Heel to shin Supine position, place heel on opposite knee and run it down to ankle; straight line without slipping from leg Sensory System Pain: Sharp/dull Broken tongue blade; apply point or blunt end 2 sec. apart; distal to core Temperature If pain sensation abnormal, apply cool/warm Light touch Cotton wisp brushed across skin; distal to core Vibration Tuning fork base to great toe/finger; distal to core Position (Kinesthesia) Move finger/toe up or down; hold by sides Tactile Discrimination: Fine touch Stereognosis Ability to recognize items by feeling form Graphesthesia Ability to “read” number traced in palm Two point discrimination Ability to distinguish two simultaneous pin points on skin Extinction Ability to sense both sides of body being touched Point Location Ability to locate sensation of touch Deep Tendon Reflexes Measurement reveals if reflex arc is intact at specific spinal levels Limb relaxed and muscle partially stretched Relaxed hold on reflex hammer; wrist snap Direct short blow onto the muscle’s insertion tendon Compare bilaterally Reflex grading scale 4+ 3+ 2+ 1+ 0 Very brisk, hyperactive More brisk than average Average Diminished, Low normal No response If reflex difficult to elicit: encourage relaxation, reposition, increase strength of blow Deep Tendon Reflexes Biceps reflex (C5-C6) Support forearm, place thumb on biceps tendon, strike thumb Contraction of biceps and flexion of the forearm Triceps Reflex (C7-C8) Holding under upper arm, suspend arm at 90 degrees Strike triceps tendon directly above elbow Extension of the forearm Brachioradialis Reflex (C5-C6) Hold thumbs to suspend forearms; strike 2-3 cm above the radial styloid process Flexion and supination of the forearm Quadriceps Reflex: Knee jerk (L2-L4) Lower legs dangle freely; strike tendon just below the patella Extension of lower leg and contraction of quadricep muscles Achilles Reflex (L5-S2) Knee flexed and hip externally rotated; hold foot in dorsiflexion, strike the Achilles tendon directly Plantar flexion against hand Plantar Reflex (L4-S2) Begin at heel, stroke lateral side of sole upward and inward across ball of foot (upside down ‘J’) Plantar flexion of all toes and inversion and flexion of the forefoot Babinski sign Dorsiflexion of great toe and fanning of all toes; NORMAL in infants until age two NOT normal in adults/children older than two Superficial reflexes Receptors are in the skin rather than the muscles Abdominal reflexes (Upper T8-T10, Lower T10-T12) Supine position, stroke lateral to midline Ipsilateral contraction and pulling of umbilicus toward stroke Cremasteric Reflex (L1-L2) In males, stroke inner aspect of thigh; note elevation of ipsilateral testicle Glasgow Coma Scale Standardized objective assessment that defines LOC by giving it a numeric value Eye opening Verbal Response Motor Response Reflects functional state of brain as a whole, not any particular site in brain Fully alert, optimal functioning—score 15 Comatose—score 7 or less Pupil size and response to light often performed