UNMH Hospitalist recs for hip fx
advertisement

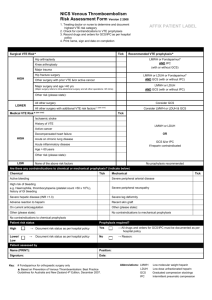
UNMH Hospitalist Section RECOMENDATIONS for ELDERLY PATIENTS WITH HIP FRACTURE 1. Order foam or alternating pressure mattress [lowers risk of pressure sores by 65-80%] 2. Operative repair within 24 – 48 hours of fracture [lowers risk of pressure sores by 55%, major post-operative complications by 75%, reduces length of stay by 2 days, lowers one year mortality] 3. Order telemetry for patients with syncope [opinion] 4. Consider regional or spinal anesthesia [lowers 30 day mortality, decreases risk of post-op DVT by 35%, decreases risk of postoperative pneumonia by 40%] 5. Prescribe perioperative prophylactic antibiotics (cephazolin, or vancomycin if cephalosporin or penicillin allergic; first dose to be given less than two hours before surgery; duration no more than 24 hours) [lowers risk of postoperative wound infection by 65%, risk of postoperative UTI by 35%] 6. Prescribe VTE prophylaxis for all patients (see VTE order set) [lowers risk of VTE by 40%] 7. Begin VTE prophylaxis pre-operatively (heparin or warfarin to begin day before surgery, LMW heparin not before 12 hrs before surgery) [opinion] 8. Consider extending VTE prophylaxis for 6 weeks after surgery [reduces risk of VTE occurring after discharge] 9. Avoid meperidine and propoxyphene for pain [opinion] 10. Discontinue Foley within 24 hours of surgery, use intermittent catheterization for urinary retention [returns voiding to normal 4 days sooner that use of indwelling catheter] 11. Mobilize within 24 hours [decreases length of stay and improves functional status] 12. Order gait training and occupational therapy [decreases risk of recurrent falls by 25%] 13. Consider discharge to an organized rehabilitation unit, especially in patients with mild dementia [decreases risk of institutionalization] 14. Begin calcium (1200 mg daily) and vitamin D (400 – 800 international units daily) as soon as eating [opinion] 15. Unless contraindicated, start bisphosphonates before discharge [opinion] [Specific recommendations followed by evidence-based reason; or opinion.] Evidence-based literature includes Beaupre LA, Jones CA, Saunders LD, Johnston DW, Buckingham J, Majumdar SR. Best practices for elderly hip fracture patients. A systematic overview of the evidence. J Gen Intern Med. 2005 Nov;20(11):1019-25; Chilov MN, Cameron ID, March LM, Australian National Health and Medical Research Council. Evidence-based guidelines for fixing broken hips: An update. Med J Aust. 2003 Nov 3;179(9):489-93; Huddleston JM, Whitford KJ. Medical care of elderly patients with hip fractures. Mayo Clin Proc. 2001 Mar;76(3):295-8; Geerts WH; Bergqvist D; Pineo GF; Heit JA; Samama CM; Lassen MR; Colwell CW. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008 Jun;133(6 Suppl):381S-453S. V1. 2009May05