Supplementary Material for “Genome

1
Supplementary Materials to:
Genome-wide association study of antipsychotic induced QTc interval prolongation
Karolina Åberg (PhD) a *; Daniel E. Adkins (PhD) a ; Youfang Liu (PhD) b ; Joseph L.
McClay (PhD) a
; József Bukszár (PhD) a
; Peilin Jia (PhD) c
; Zhongming Zhao (PhD) c
;
Diana Perkins (MD) d
; Scott Stroup (MD)
e
; Jeffrey A. Lieberman (MD) e
; Patrick F.
Sullivan (MD) b, f
; Edwin J.C.G. van den Oord (PhD) a a Center for Biomarker Research and Personalized Medicine, School of Pharmacy, Medical College of
Virginia of Virginia Commonwealth University, Richmond VA 23289, USA; b Departments of Genetics,
Psychiatry and Epidemiology, University of North Carolina at Chapel Hill, NC 27599, USA; c Departments of Biomedical Informatics, Psychiatry and Cancer Biology, Vanderbilt University Medical Center, TN
37203, USA; d Department of Psychiatry, University of North Carolina at Chapel Hill, NC 27514, USA; e
Department of Psychiatry, Columbia University, New York, NY 10032, USA; f Department of Medical
Epidemiology and Biostatistics, Karolinska Institutet, 17177 Stockholm, Sweden.
*Correspondence to: Karolina Åberg, Center for Biomarker Research and Personalized Medicine, School of Pharmacy, Medical College of
Virginia of Virginia Commonwealth University, 1112 East Clay Street,
P.O. Box 980533, Richmond, VA 23298.
Tel: +1 804-628 3023, fax: +1 804-628 3991, e-mail: kaaberg@vcu.edu
Content:
Estimating treatment effects for antipsychotic-induced QTc prolongation page 2-8
Figure S1 page 9
2
Estimating treatment effects for antipsychotic-induced QTc prolongation
To develop measures of the effects of antipsychotic usage on heart rate-adjusted
QT interval (QTc), we employed a mixed model approach conceptualizing individual differences in drug response as random effects. Specifically, we used a multi-step model fitting procedure to: 1) determine the correct functional form of longitudinal, antipsychotic-induced change in QTc and 2) screen 27 potentially relevant covariates to identify those that improve the precision of the treatment effect measures. After identifying the optimal functional form and covariate set, we estimated linear mixed models predicting QTc with fixed and random effects for each of the following drugs: olanzapine, perphenazine, quetiapine, risperidone and ziprasidone, as well as fixed effects for selected covariates.
Linear mixed models are a generalization of linear regression allowing for the inclusion of individual-level random deviations (effects) other than those associated with the overall residual term. In matrix notation, y = Xβ + Zu +
ε
Eq. 1 where y is the n ×
1 vector of responses, X is a n × p
design/covariate matrix for the fixed effect β , and Z is the n × q design/covariate matrix for the random effects u. The n
×
1 vector of residuals
ε,
is assumed to be multivariate normal with mean zero and variance matrix
σ e
2
I n
.
The fixed portion, Xβ , is equivalent to the linear predictor of OLS regression. For the random portion, Zu +
ε
, it is assumed that the u has variance-covariance matrix G and that u is orthogonal to ε so that
Var
u
G
0
0 e
2
I n
Eq. 2
3
The random effects u are not directly estimated (although, as described below, they are predicted), but instead are characterized by the elements of G , known as the variance components, that are estimated along with the residual variance
σ e
2
. Considering Zu +
ε the combined error, we see that y is multivariate normal with mean Xβ and n × n variance-covariance matrix
V = ZGZ ’+ σ e
2 I n
Eq. 3
In the current analysis, our model fitting procedure begins with identifying the correct functional form of longitudinal, antipsychotic-induced change in QTc. That is, we determine how long it takes for antipsychotic-induced QTc change to reach its maximum and plateau. This is vital to developing high-quality measures of treatment effects, because to the extent the assumed functional form deviates from the actual one, noise is introduced into the measure and the power to detect associations in the GWAS is proportionately diminished. For this reason, we estimate a series of models in which the number of days until antipsychotic-induced QTc change plateaus varies systematically, beginning with a model that assumes maximal response at day 1, and then increasing the number of days, in 30 day increments, until the final model in which no plateau is observed (i.e., constant linear change throughout the trial).
This procedure is achieved using the equation: y ij
=
β
0
+
β
1
D ij
+ u
0i
+ u
1i
D ij
+ e ij where i and j denote the subject and assessment levels, respectively; y is the QTc for subject i at assessment j ; β
0
is the overall sample intercept; β
1 is the sample mean
Eq. 4 coefficient (i.e., fixed effect) of antipsychotic treatment; u
0i
is the subject-specific deviation (i.e., random effect) from that overall sample intercept; u
1i
is the random effect
4 of the mean antipsychotic treatment coefficient; e ij
is the residual for subject i at assessment j . Most importantly, D is a variable that describes how long the subject has been on the current antipsychotic. D is recoded in each model of the series to specify a different number of days until maximal response (i.e., a plateau) is achieved. Thus, for the first model in the series, which assumes maximal effect at day 1, D is coded 0 if the subject isn’t on the antipsychotic, 1 at day 1, and 1 each day thereafter. In the second model which assumes maximal effect at day 31, D is coded 0 if the subject isn’t on the antipsychotic, 1 if they have been on for 1 day, 2 for 2 days, and so on, until day 31, after which D is coded equal to 31 for the duration of treatment with that antipsychotic.
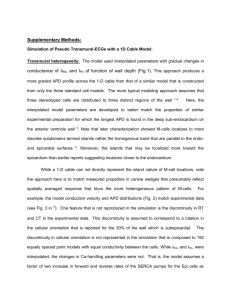
Indices of model fit (log likelihoods) were collected for each model in the D series, and then the function created by these values was minimized to determine the optimal response functional form. Figure S1 presented the graphed log likelihood values for each outcome with the optimal plateau value, 291, marked with a red vertical line.
After determining the optimal functional form of the antipsychotic treatment effects, we then screened 27 covariates (shown in Table S1) to identify those that improved the precision of the treatment effects. More specifically, we sought covariates that accounted for error in the model, but did not mediate the treatment effects. Thus, we employed a decision rule specifying that covariate must: 1) explain a significant among of variance in the outcome (i.e., coefficient p -value > .05), and 2) reduce the residual
Figure S1. Identifying optimal plateau function form for antipsychotic-induced QTc change (i.e. treatment effects)
5
0 150 300 450
Days until QTc change stabilizes
600 variance (VAR( e )) significantly more than the treatment effect variance (VAR( u
1
)). The
27 covariates considered were selected from four primary domains: 1) Design characteristics – which captured the characteristics of the trial structure such as what phase the subject was currently in, the total number of days the subject had been in the trial, and when a given phase ended; 2) Clinical factors – including the number of years since first antipsychotic treatment, number of year since diagnosis and experience of current exacerbation; 3) Socio-demographic information – this included information on age, gender, education, race and employment; 4) Confounding medications – metabolic relevant medications such as treatments for hyperlipidemia, diabetes, hypertension and weight gain. Two covariates—“treatment inadequate” and “in trial”—were found to improve precision and were retained.
Table S1. List of screened covariates
6
Design characteristics
Visit day
In trial
Phase 1a
Phase 1b
Phase 2
Phase 3
Follow up
End of Phase
End of Phase 1a
End of Phase 1b
End of Phase 2
Clinical information
Switched drug
Treatment inadequate
Yrs since 1st antipsychotic
Yrs since 1st treatment
End of Phase 3
Precision-enhancing covariates are marked in bold.
Sociodemographics
Gender
Age
White
Black
Hispanic
Education
Employment
Confounding meds
Weight gain med
Diabetes med
Hyperlipidemia med
Hypertension med
After determining the proper functional form of the over-time treatment effects and identifying the precision-enhancing covariates, we then output the random effects for each of the CATIE trial antipsychotics, yielding a total of five random effect measures.
These measures quantify the deviation of each subject’s antipsychotic-induced QTc change from the overall sample mean change and thus, serve as our treatment effect measures in the subsequent GWAS. Specifically, they are estimated with the equation: y ij
=
β
0
+
β
1
D kij
+
β
2
O kij
+
β l+2
C lij
+ u
0i
+ u
1i
D kij
+ u
2i
O kij
+ e ij
Eq.5 where i and j denote the subject and assessment levels, respectively; y is QTc for subject i at assessment j ;
β
0
is the overall sample intercept; D is the specific trial antipsychotic modeled, indexed 1-6 by k ; β
1 is the sample mean coefficient (i.e., fixed effect) for antipsychotic k ; O is all antipsychotics other than k; β
2 is the fixed effect for O; l indexes the number of covariates C included in the model;
β l+2 are the fixed effects for C l
; for u
0i is the subject-specific deviation (i.e., random effect) from that overall sample intercept; u
1i
is the random effect of D k
; u
2i
is the random effect of O k
; e ij
is the residual for subject i
7 at assessment j . The parameter of interest, u
1i
, may be more intuitively described as the subject-specific effect of antipsychotic k on QTc.
Models of the general form shown in Eq. 5 were estimated five times, once for each drug. The five drug effects were not estimated simultaneously because there were not sufficient repeated observations to identify a model with so many random parameters.
In previous research on CATIE outcomes with sufficient repeated assessments to allow simultaneous estimation of all trial drug random effects (e.g. BMI), the treatment effects were found to be virtually identical ( r > .96) to those in which each drug’s treatment effect was estimated separately.
In each model, the covariance structure of the three random effects was modeled as independent:
u u u
0i
1i
2i
~ N(0, G) with G =
0
0
2 u 0
2 u 1
0
2 u 2
Eq.6
Thus, the random parameters are multivariate normal distributed with means of zero and variance-covariance matrix G . The variances of the parameters are on the diagonal and the covariances, constrained equal to zero, are in the off-diagonal cells of G . The residual is assumed to be normally distributed with a mean of zero and variance of σ 2 e
.
Because random effects are not directly estimated by the mixed model, they must be predicted in an additional post-estimation step. Best linear unbiased predictors
(BLUPs) of the random effects u were obtained as
~
G Z
~
V
1
( y
X
ˆ
) Eq.7
8
~ where G
~ and V are G and V with estimates of the variance components plugged in. The
EM algorithm was used for maximum likelihood estimation as described by Pinheiro and
Bates (1).
References
1. Pinheiro JC, Bates DM: Mixed-effects models in S and S-plus. New York, NY:
Springer, 2000.
Figure S1.
Regional plot of SNPs located on chromosome 6p25.2.
9
1.
The genome-wide significant SNP (rs4959235) in SLC22A23 is indicated in blue. The locations of the two genes (PSMG4 and SLC22A23) in the regions are shown as green arrows. The directions of the arrows indicate the direction of the genes.
Pinheiro JC, Bates DM: Mixed-effects models in S and S-plus. New York, NY:
Springer, 2000.