Junior Marsipan
advertisement

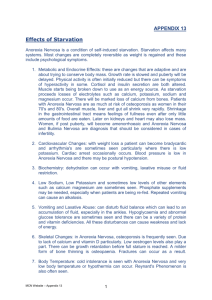
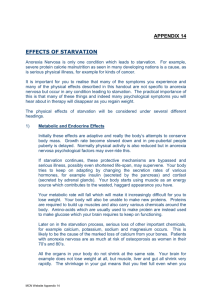
Medical Assessments in Adolescence Junior MaRSiPAN Dr Mark Anderson Background • 0.5% of adolescent females have anorexia nervosa • 1-5% of adolescent females have bulimia nervosa • 5-10% of eating disorders occur in males • Early recognition and intervention are thought to improve outcome Whose problem is it? • Psychiatric disorder • Significant physical issues – – – – Starvation Growth Re-feeding syndrome Long term sequelae • Acute medical issues • Safety in community • Multi-disciplinary approach What can paediatricians offer? • Medical assessment – Junior MaRSiPAN – Determine “risk” – Investigations • Admission – – – – At risk Medical complications Risk of re-feeding syndrome Break the cycle, relieve pressure Newcastle routes of referral • CYPS (CAMHS) • GP • Emergency department • Mostly via myself Initial assessment • Full history and medical assessment • Blood tests and ECG • Risk assessment according to Junior MaRSiPAN – Management of Really Sick Patients with Anorexia Nervosa (Junior!) Junior Marsipan Risk Assessment • Semi-objective • Aims to give an overall assessment of risk • It is not: – A scoring system – Validated to predict need for admission, specific management or outcome • Needs to be seen as part of the gestalt of assessment Measurements • Percentage median BMI – – – – >85% 80-85% 70-80% <70% • Recent weight loss – – – – No change Up to 500g/week for 2 weeks 500-999g/week for 2 weeks >1kg for 2 weeks Cardiovascular 1 • Heart rate (awake) – >60 bpm – 50-60 bpm – 40-50 bpm – <40 bpm • Cool peripheries Cardiovascular 2 • Blood pressure – Normal – <2nd centile – <0.4th centile • Syncope – No symptoms – Presyncopal symptoms – Occasional syncope with postural drop in BP – Recurrent syncope with marked postural drop Cardiovascular 3 • Arrhythmia – Normal – Irregular heart rhythm • ECG changes – QTc <450ms – QTc <450ms and taking QT prolonging medication – QTc >450ms – QTc >450ms and evidence of arrhythmia or electrolyte disturbance Other physiological parameters • Hydration – Not dehydrated – Mild dehydration – Moderate dehydration or peripheral oedema – Severe dehydration • Temperature – <36°C – <35°C Biochemical abnormalities – Hypophosphataemia – Hypokalaemia – Hyponatraemia – Hypocalcaemia – Severe abnormalities of above Calorie intake • Moderate restriction or bingeing • Severe restriction (<50% of requirement) • Purging • Acute food refusal or <600kcal/day Activity & exercise • No uncontrolled exercise • Mild uncontrolled exercise (<1h/day) • Moderate uncontrolled exercise (1-2h/day) • Severe uncontrolled exercise (>2h/day) Muscular weakness • SUSS test – No difficulty – Unable to get up without noticeable difficulty – Unable to get up without using arms – Unable to get up at all Engagement with management plan • Some insight and motivation, not ambivalent • Some insight and motivation, but ambivalent • Poor insight and motivation; parents unable to implement meal plan • Violent when parents try to implement plan; parental violence Co-morbidities • Deliberate self harm • Suicidal ideation • Other major psychiatric co-diagnosis Outcomes of medical assessment • Mostly blue-green, no red – Outpatient follow-up • More amber, or some red – Admission for period of assessment • No definite “admission criteria” Admission • Decision re: feeding method • Dietitian input – daily • Set nursing guidance – obs, bed rest, “rules” • Make plan with YP (and family) • Daily review – close medical monitoring • Regular input from CYPS • Plan discharge What we have learnt… • • • • • AN is very difficult The illness makes it hard Staff often feel manipulated Nursing time is a major issue 16-18 year olds fall through the gaps Longer term issues • General health • Bone health Bones • Low bone mineral density • Critical time • Risk of later osteoporosis • Back pain • Chronic ill health Bones • • • • Nutrition Hypogonadism Relative hypercortisolaemia Low IgF1 • Weight and nutrition improve BMD • Residual defect left Bones • Possible options – OCP (high dose OE) – Bisphosphonates – Low dose OE – Transdermal OE – Calcium/Vitamin D Toronto study 2011 • Randomised placebo controlled study • 40 girls normal weight - controls • 110 girls AN – randomised – OE + – OE – • OE transdermal 100mcg patch twice weekly OR escalating doses of oral OE 3.75mcg daily increasing over 18 months • OE + given medroxyprogesterone 2.5 mg daily for 10 days every month • OE – placebo patch and placebo medroxyprogesterone • Controls followed for 18 months no intervention • ALL had calcium carbonate and Vit D Results BMD change Results • • • • • No change in weight No change in lean body mass No change in percentage fat mass No change in BMI No change in IgF1 Recommendations • DEXA scan – ?when • Commence OE replacement – ?when – Who should do this/monitor progress – What happens >18 years of age – What about the boys? Conclusions • • • • • • Acute management Good liaison Easy for <16 year old Need to support 16-18 year olds Long term input Bones and future health Questions? • • • Junior MARSIPAN: MAnagement of Really Sick Patients under 18 with Anorexia Nervosa – College report CR 168, January 2012 RCPSYCH Norrington, Stanley, Tremlett, Birrell. Medical management of acute severe anorexia nervosa Arch Dis Child Educ Pract Ed 2012;97:48-54 Physiologic Estrogen Replacement Increases Bone Density in Adolescent Girls With Anorexia Nervosa. Misra M, Katzman D, Miller K , Mendes N, Snelgrove D, Russell M, Goldstein, Ebrahimi M, Clauss L, Weigel T, Mickley D, Schoenfeld D , Herzog D, Klibanski A. Journal of Bone and Mineral Research, Vol. 26, No. 10, October 2011, pp 2430–2438