Post-infectious Bronchiolitis Obliterans
advertisement

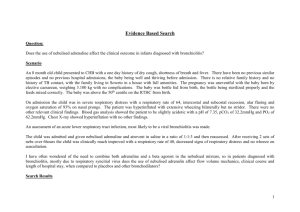
Post-infectious Bronchiolitis Obliterans Alejandro Teper, MD and Alejandro Colom, MD Respiratory Center of the Ricardo Gutiérrez Children’s Hospital of Buenos Aires, Argentina. Bronchiolitis obliterans (BO) is an uncommon and severe form of chronic obstructive lung disease in children that results from an insult to the lower respiratory tract. Published reports have stated that bronchiolitis obliterans has been known to occur after Stevens-Johnson syndrome, as a complication of graft versus host disease in bone marrow transplant recipients, and as a manifestation of chronic graft rejection in lung transplant recipients. In many parts of the world, however, bronchiolitis obliterans is most commonly seen in children after severe viral lower respiratory tract infections. A number of respiratory viruses, especially adenovirus (AV), have been associated with severe lung injury that can lead to bronchiolitis obliterans. Bronchiolitis obliterans is characterized by partial or complete occlusion of the lumens of terminal and respiratory bronchioles by inflammatory and fibrous tissue. It is interesting to see the similarity of pathological findings in patients of different etiologies, suggesting that bronchiolitis obliterans would be the final common pathway of response to different injuries to the lower respiratory tract. Bronchiolitis obliterans could be divided pathologically into two major categories. The first is proliferative BO (also called pure-type BO), characterized by obstruction of the airway lumen by polyps of granulation tissue. When this granulation tissue extends into the alveoli, the lesion is called bronchiolitis obliterans with organizing pneumonia (BOOP). The second category is constrictive BO, which is characterized by peribronchiolar fibrosis with different degrees of lumen narrowing. Post-infectious BO is characterized histologically mainly by a constrictive pattern, with variable degrees of inflammation and airway obliteration. Other signs of airway disease, such as bronchiolar inflammation, mucostasis, macrophage accumulation and bronchiolar distortion and dilatation, were frequently reported in these patients. The histological analysis of lung biopsies in BO is limited by the multifocal pattern of the disease. Post-infectious bronchiolitis obliterans has commonly been observed after viral infections. A number of respiratory viruses, including respiratory syncytial virus (RSV), parainfluenza, influenza and especially adenovirus (AV), have been associated with severe lung injury leading to BO. Other etiologies include mycoplasma, measles, legionella, pertussis and human immunodeficiency virus-1. Cytomegalovirus infection in lung allograft transplantation has also been suggested as being associated with the subsequent appearance of BO. We performed a case-control study that included 109 cases (with bronchiolitis followed by bronchiolitis obliterans) and 99 controls (patients with bronchiolitis who did not develop bronchiolitis obliterans). The two main factors associated with the development of bronchiolitis obliterans were adenovirus bronchiolitis (odds ratio (OR) 49) and mechanical ventilation (OR 11). Although mechanical ventilation was a significant risk factor for post-infectious BO, the results do not indicate whether it causes injury to the lung that increases the risk for developing postinfectious BO or whether it merely serves as an indicator of severity of illness. The central role of AV in the development of postinfectious BO has been well documented and in our cohort is present in 70–80% of post-infectious BO patients. Since 1984 a new genotype of adenovirus, AV7h, has stood out as the most virulent serotype, but other AVs such as 3, 5 and 21 also were reported to cause BO. Patients with severe AV infection have been shown to have immune complexes containing AV antigen in the lung, as well as increased serum levels of interleukin-6, interleukin-8, and tumor necrosis factor (TNF-α). The susceptibility to develop bronchiolitis obliterans seems to be associated with the geographical origin of the human groups studied. Child populations from New Zealand, central Canada, Alaska and South America exhibit a higher incidence of post-infectious bronchiolitis obliterans than populations from Europe and other American regions. Recent studies developed in Argentine Amerindians with post-adenoviral BO show that the HLA haplotype DR8-DQB1*0302 and the Native American ethnic ancestry, determined by mtDNA markers, were increased in the affected patients. Although the data are limited, these previous studies suggest that the host immunological response may play an important role in the severity of adenoviral respiratory infections as well as the subsequent development of BO in selected populations. In our cohort of post-infectious BO patients, illness occurred in very young infants, younger than six months, but our findings did not show that age was a risk factor for developing postinfectious BO. Initially, these patients present with symptoms that do not differ from a typical RSV bronchiolitis. During the admission examination, most patients are found to have severe airway obstruction with hypoxemia and in many cases require mechanical ventilation. Physical findings are usually nonspecific. Expiratory wheezing and occasional crackles may be heard on chest auscultation. When an AV infection is detected and the patients do not get better after three weeks, BO should be suspected. After patients’ conditions have become stable they still show persistently high respiratory rates, rigid thorax, wheeze and productive cough. Oxygen saturation is often lower than normal. Other patients who initially contracted intranosocomial AV pneumonia with severe respiratory compromise (accessory muscle use and crackles) show similar development and require intensive care and lengthy hospitalization. Chest X-rays in BO patients are nonspecific but show air trapping, atelectasis, peri-bronchial thickening and honeycombing (Figure 1). Some patients show unilateral lung/lobe involvement, with hyperlucent and small lung, known as Swyer-James or MacLeod syndrome, due to loss of the pulmonary vascular structure and air trapping. Lung perfusion scans show perfusion defects, with lobar, segmental, or subsegmental pattern. Comparing lung perfusion scans with chest radiographs, the defects on lung scans correspond to areas with more prominent abnormalities, such as bronchial wall thickening and bronchiectasis. Lung perfusion scans cannot describe the nature of bronchopulmonary abnormalities; however, this examination provides an objective evaluation regarding the extent, distribution and severity of bronchopulmonary lesions. The most characteristic signs of BO with High-resolution CT (HRCT) are areas of mosaic attenuation pattern due to shunting of blood away from the under-ventilated to the normally ventilated lung, where perfusion is reduced in areas of decreased parenchyma attenuation due to hypoxic pulmonary vasoconstriction (Figure 2). Other signs include air trapping, especially on expiratory CT, and bronchial abnormalities. Air trapping, as detected on expiratory HRCT, has been described as the most sensitive and accurate radiological indicator of BO in the lung transplant population. Infant pulmonary function in post-viral BO shows severe and fixed bronchial obstruction decreased pulmonary distensibility and increased airway resistance. These patients have more severely affected V’maxFRC than in other diseases such as bronchopulmonary dysplasia or asthma which, even in their most severe forms, usually respond to bronchodilators. These findings might represent the functional expression of the histopathological damage of bronchiolitis obliterans. Another factor associated with BO is gastroesophageal reflux (GER), which itself is relatively common and may adversely affect lung function. Extensive studies in children have not been carried out to confirm this complication, although our experience suggests that GER needs to be investigated in postinfectious BO patients. When other causes of chronic lung disease have been eliminated, the patient’s clinical history, chest radiographies and HRCT images are sufficient in most cases to confirm the diagnosis and to differentiate post-infectious BO from other pulmonary disorders. These clinical evaluations should be considered in tandem with the functional pattern in post-infectious BO. Usually it is not accessible to perform an Infant PFT. To develop and to validate a clinical prediction rule to diagnose children under 2 years old with post viral bronchiolitis obliterans, we have designed a retrospective cohort study of children with chronic lung disease using multiple objectively measured parameters readily available in most medical centers. We compared a group of confirmed BO patients under 2 years old (clinical history, lung function tests and CT scan compatible) with infants and young children with other confirmed chronic lung diseases such as primary ciliary diskinesia (PCD), cystic fibrosis (CF) and bronchiectasis of different etiologies than BO, PCD and CF. BO diagnosis was considered the dependent variable. Predictive variables were: a) “clinical history”, defined as a previous healthy child, who suffered a severe viral infection and remained with chronic respiratory symptoms and hypoxemia (SaO2 <92%) for more than 60 days; b) antecedent of “adenoviral infection”; c) “mechanical ventilation” requirement; and three HRCT patterns: d) “mosaic pattern”; e) “atelectasis” and f) “bronchiectasis”. The BO-Score (area under ROC curve= 0.96; 95% CI, 0.9–1.0%) was developed by assigning points to the following variables: typical clinical history (four points), adenovirus infection (three points), and highresolution computed tomography with mosaic perfusion (four points). A Score equal or higher than 7, predicted the diagnosis of BO with a specificity of 100% (95% CI, 79–100%) and a sensitivity of 67% (95% CI, 47–80%). If doubt persists about the diagnosis, a lung biopsy may be needed. Most patients with post-infectious BO require oxygen supplementation for nearly a year after discharge from the initial hospital admission. Readmission to hospital will probably be required for subsequent infections of the lower respiratory tract. In older children, only few patients require oxygen supplementation. Spirometry test results show evidence of airflow limitation, and pletismography demonstrates gas trapping with normal or high total lung volumes. Therefore, pulmonary function remains severely impaired, showing a moderate-severe obstructive pattern. Children with postinfectious BO have moderate compromise of mechanics as measured by forced oscillation, with high resistance and low compliance. In most patients, perfusion defects shown by the initial lung scans persisted and occasionally increased. Clinical improvement during the disease process may be due to the growth of the lungs in these children, and probably does not indicate regression of the pathology in the small airways. The overall prognosis of pulmonary function was poor in the majority of the cohort studies published. Mortality and morbidity rates associated with post-infectious BO remain uncertain. Prognosis in an individual patient may relate to several factors, including length of oxygen requirement, mechanical ventilation requirements, severity of re-infections of the lower respiratory tract and probably others. Large case-control studies will be necessary in order to address this knowledge gap. The majority of evidence suggests that BO is immune mediated, so therapeutic interventions have focused on the suppression of the inflammatory response. Anti-inflammatory therapy such as corticosteroids, chloroquine and hydroxylchloroquine has been tried in small clinical trials and case reports with minimal success. Because bronchiolitis obliterans is so rare, controlled and randomized therapeutic clinical trials have been impossible to perform. Although multiple cytokines and chemokines have been identified in the pathogenesis of BO, tumour necrosis factor (TNF-α) seems to play a central role in the inflammatory reaction and enhances fibroblast proliferation. A case report describes successful treatment of BO in a bone marrow transplant patient with TNF-α blockade (Infliximab). Other studies suggest a potential role for maintenance of macrolide therapy in the treatment of bronchiolitis obliterans where the anti-inflammatory properties and ability to reduce inflammatory mediators of interleukin IL-8, TNF-α, and IL-1ß may play a role. When the disease is well established, however, the principal treatment is supportive and includes bronchodilators, chest physical therapy, antibiotics for acute respiratory infections, and in some patients, diuretics. Gastroesophageal reflux has been increasingly recognized as a factor that may significantly contribute to BO, so when it is recognized, treatment is warranted. Post-infectious BO has been reported in limited areas, where its impact is profound. Although research has identified the risk factors that can lead to post-infectious BO, knowledge about factors inherent to the population, such as a genetic predisposition to develop the disease is still scarce. Clinical trials of potential therapeutic agents should be multicentre studies in order to include a significant number of patients. Important factors to consider include the ideal timing, dosage and best choice of immunosuppressive agent to avoid the development of the disease. References 1. Hardy KA, Schidlow DV, Zaeri N. Obliterative bronchiolitis in children. Chest 1988; 93: 460– 466. 2. Boehler A, Estenne M. Post-transplant bronchiolitis obliterans. Eur Respir J Monogr 2003; 26: 158–178. 3. Jaramillo A, Fernandez FG, Kuo EY, Trulock EP, Patterson GA, Mohanakumar T. Immune mechanisms in the pathogenesis of bronchiolitis obliterans syndrome after lung transplantation. Pediatr Transplant Feb. 2005. 4. Colom AJ, Teper AM, Vollmer WM, Diette GB. Risk factors for the development of bronchiolitis obliterans in children with bronchiolitis. Thorax 2006; 61: 503–506. 5. Zhang L, Irion K, Kozakewich H et al. Clinical course of postinfectious Bronchiolitis obliterans. Pediatr Pulmonol 2000; 29: 341–350. 6. Castro-Rodriguez J, Daszenies C, Garcia M, Meyer R, Gonzales R. Adenovirus pneumonia in infants and factors for developing bronchiolitis obliterans: a 5 year follow-up. Pediatr Pulmonol 2006; 41: 947–953. 7. Yalçına E, Dogrua D, Haliloglub M, Özçelika U, Kipera N, Göçmena A. Postinfectious bronchiolitis obliterans in children: clinical and radiological profile and prognostic factors. Respiration 2003; 70: 371–375. 8. Chang A, Masel J, Masters B. Post-infectious bronchiolitis obliterans: clinical, radiological and pulmonary function sequelae. Pediatr Radiol 1998; 28: 23–29. 9. Becroft DMO. Bronchiolitis obliterans, bronchiectasis, and other sequelae of adenovirus type 21 infection in young children. J Clin Pathol 1971; 24: 72–82. 10. Krasinski K. Severe respiratory syncytial virus infection: clinical features, nosocomial acquisition and outcome. Pediatr Infect Dis J 1985; 4: 250–257. 11. Welliver R, Wong D, Sun M et al. Parainfluenza virus bronchiolitis. Am J Dis Child 1986; 140: 34–40. 12. Laraya-Cuasay LR, DeForest A, Huff D et al. Chronic pulmonary complications of early influenza virus infection in children. Am Rev Respir Dis 1977; 116: 617–625. 13. Simila S, Linna O, Lanning P et al. Chronic lung damage caused by adenovirus type 7: a ten year follow up study. Chest 1981; 80: 127–§31. 14. Wiebicke W, Seidenberg J. Obliterating bronchiolitis following measles. Pneumologie 1990; 44: 1220–1222. 15. Sato P, Madtes DK, Thorning D, Albert RK. Bronchiolitis obliterans caused by Legionella pneumophila. Chest 1985; 87; 840–842. 16. Trimis G, Theodoridou M, Mostrou G, Kakavakis K. Swyer-James (MacLeod’s) syndrome following pertussis infection in an infant. Scand J Infect Dis 2003; 35: 197–199. 17. Diaz F, Collazos J, Martinez E, Mayo J. Bronchiolitis obliterans in a patient with HIV infection. Respir Med 1997; 91: 171–173. 18. Kajon A, Mistchenko A, Videla C et al. Molecular epidemiology of adenoviruses associated with acute lower respiratory infections of children in the south cone of South America (1991–1994). J Med Virol 1996; 48: 151–156. 19. Schmitz H, Wigand R, Heinrich W. Worldwide epidemiology of human adenovirus infections. Am J Epidemiol 1983; 117: 455–466. 20. Kajon A, Mistchenko A, Videla C et al. Molecular epidemiology of adenoviruses associated with acute lower respiratory infections of children in the south cone of South America (1991–1994). J Med Virol 1996; 48: 151–156. 21. Purkayastha A, Su J, McGraw J et al. Genomic and bioinformatics analyses of HAdV-4vac and HAdV-7vac, two human adenovirus (HAdV) strains that constituted original prophylaxis against HAdV-related acute respiratory disease, a reemerging epidemic disease. J Clin Microbiol 2005; 43: 3083–3094. 22. Wadell G, Varsanyi TM, Lord A, Sutton RN. Epidemic outbreaks of adenovirus 7 with special reference to the pathogenicity of adenovirus genome type 7b. Am J Epidemiol 1980; 112: 619–628. 23. Mistchenko AS, Lenzi HL, Thompson FM et al. Participation of immune complexes in adenovirus infection. Acta Paediatr 1992; 81: 983–988. 24. Mistchenko AS, Diez RA, Mariani A et al. Cytokines in adenoviral disease in children: association of interleukin-6, interleukin-8, and tumor necrosis factor alpha levels with clinical outcome. J Pediatr 1994; 124: 714–720. 25. Lang W, Howden C, Laws J et al. Bronchopneumonia with serious sequelae in children with evidence of adenovirus type 21 infection. BMJ 1969; 1: 73–9. 26. Wenman W, Pagtakhan R, Reed M et al. Adenovirus bronchiolitis in Manitoba. Epidemiologic, clinical and radiologic features. Chest 1982; 81: 605–609. 27. Teper AM, Marcos CY, Theiler G, Colom AJ, Fainboim L. Association between HLA and the incidence of bronchiolitis obliterans (BO) in Argentina. Am J Respir Crit Care Med 2004; 169: 382 (Abstract). 28. Teper A, Colom A, Bailliet G, Martnez-Marignac V, Bianchi N. Association between the incidence of bronchiolitis obliterans (BO) in Argentine children and their native-american maternal and paternal lineage. Am J Respir Crit Care Med 2003; 167: 998. (Abstract) 29. Kajon A, Gigliotti A, Harrod K. Acute inflammatory response and remodeling of airway epithelium after subspecies B1 human adenovirus infection of the mouse lower respiratory tract. J Med Virol 2003; 71: 233–244. 30. Leong MA, Nachajon R, Ruchelli E et al. Bronchitis obliterans due to Mycoplasma pneumonia. Pediatr Pulmonol 1997; 23; 375–338. 31. Massie R, Armstrong D. Bronchiectasis and bronchiolitis obliterans post respiratory syncytial virus infection: think again. J Paediatr Child Health 1999; 35: 497–498. 32. Hirschheimer M, Silva P, Giudici R et al. Simultaneous viral infection and childhood bronchiolitis obliterans. Braz J Infect Dis 2002; 6: 146–148. 33. Swyer PR, James GCW. A case of unilateral pulmonary emphysema. Thorax 1953; 8: 133–136. 34. MacLeod VVM. Abnormal transradiancy of one lung. Thorax 1954; 9: 147–153. 35. Leung A, Fisher K,Valentine V, Girgis R, Berry G, Robbins R, Theodore J. Bronchiolitis obliterans after lung transplantation, detection using expiratory HRCT. Chest 1998; 113: 365–370. 36. Teper AM, Kofman CD, Maffey AF et al. Lung function in infants with chronic pulmonary disease after severe adenoviral illness. J Pediatr 1999; 134: 730–733. 37. Maffey A, Colom A, Kofman C, Vidaurreta S, Teper A. Longitudinal study of pulmonary function in infants with post viral chronic pulmonary disease (PCPD). Am J Respir Crit Care Med 1996; 153: 498. (Abstract) 38. Colom AJ, Maffey A, Navarra F, Teper A. Pulmonary function in children with post-viral chronic pulmonary disease (PCPD). Am J Respir Crit Care Med 2002; 163: A159. (Abstract) 39. Colom AJ, Navarra F, Kofman C, Teper A. Respiratory mechanics in children with post-viral chronic pulmonary disease (PCPD). Am J Respir Crit Care Med 2002; 163: A159. (Abstract). 40. Kim CK, Kim SW, Kim JS et al. Bronchiolitis obliterans in the 1990s in Korea and the United States. Chest 2001; 120: 1101–1106. 41. Fullmer J, Fan L, Dishop M, Rodgers C, Krance R. Successful treatment of bronchiolitis obliterans in a bone marrow transplant patient with tumor necrosis factor-α blockade. Pediatrics 2005; 116: 767–770. 42. Gerhardt S, McDyer J, Girgis R, Conte J, Yang S, Orens J. Maintenance azithromycin therapy for bronchiolitis obliterans syndrome. Results of a pilot study. Am J Respir Crit Care Med 2003; 168: 121–125. 43. Colom A and Teper AM. Clinical prediction rule to diagnose post-infectious bronchiolitis obliterans in children. Pediatr Pulmonol 2009; 44:1065–1069. Figures Figure 1: Chest radiograph of patient with post-infectious BO, with air trapping, atelectasis and bronchiectasis. Figure 2: CT scan of patient with post infectious BO, with mosaic attenuation pattern, atelectasis and bronchiectasis.