Age Length of stay Bronchiolitis admissions among term and
advertisement

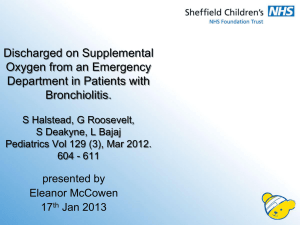
Creating a birth cohort to examine RSV bronchiolitis hospital admission rates among term and preterm infants in England Joanna Murray 1, Alex Bottle 1, Mike Sharland 2, Neena Modi 3, Paul Aylin 1, Azeem Majeed 1 and Sonia Saxena1 1 Department of Primary Care and Public Health, Imperial College London, UK 2 Paediatric Infectious Diseases Unit, St George’s Hospital NHS Trust, London, UK 3 Section of Neonatal Medicine, Department of Medicine, Imperial College London On behalf of the Medicines for Neonates Investigator Group: Neena Modi, Peter Brocklehurst, Jane Abbott, Kate Costeloe, Elizabeth Draper, Azeem Majeed, Jacquie Kemp, Deborah Ashby, Alys Young, Stavros Petrou Results All bronchiolitis admissions Introduction • Bronchiolitis is a common respiratory illness among infants, typically caused by respiratory syncytial virus (RSV). It is usually a mild, self-limiting illness but in some infants may be more severe, requiring hospital admission.1 Birth cohort (n=296618) 7189 admissions to hospital with bronchiolitis during the first year of life • Infants known to be at high risk of severe RSV infection include those with chronic lung disease, congenital heart disease, immunodeficiency, low birth weight and those born preterm (around 8% of newborns in the UK).2-5 • Evidence from the US suggests many infants admitted to hospital with RSV infection are healthy, with no risk factors for severe RSV infection.3 • To date, no national studies have reported the disease burden at a population level in the UK. • An active immunisation against RSV is currently in phase III trials. 24.2 admissions per 1000 infants under 1 year (95% CI 23.7 to 24.8) Median age at admission = 120 days (Inter-quartile range = 61 to 209) Figure 1. Age at bronchiolitis admission 900 800 700 RSV Bronchiolitis 600 Number of 500 hospital admissions 400 Unspecified Bronchiolitis 300 Aim 200 We aimed to examine RSV bronchiolitis hospital admission rates among term and preterm infants in England. 100 0 0 1 2 3 4 5 6 7 8 9 Age at admission (in months) 10 11 12 Bronchiolitis admissions among term and preterm infants Among infants who had a bronchiolitis admission: 15% were born preterm (n =1050) 47.3 per 1000 infants (95%CI 44.4 to 50.2) Methods We developed a population-based birth cohort with follow-up to age 1 year using the Hospital Episode Statistics (HES) database. We identified individual birth records from a twelve month period (01/04/2007 to 31/03/2008), from 71 NHS hospitals across England (where >90% of their birth records contained complete recording of key variables, birth weight and gestational age) and linked to subsequent hospital admission records. 85% were born at term (n = 6139) 22.4 per 1000 infants (95%CI 21.8 to 22.9) Age Median age at bronchiolitis admission among infants born: Preterm = 136 days (IQR = 71 to 221) P < 0.001 Term = 118 days (IQR = 59 to 207) Infants were considered preterm if their gestational age at birth was less than 37 weeks, in accordance with the WHO definition of premature birth. Length of stay Median length of stay for a bronchiolitis admission among infants born: We identified emergency admissions with a primary diagnosis of bronchiolitis using the ‘J21’ ICD-10 codes. Most bronchiolitis admissions were coded with unspecific aetiology and around a third were coded as being due to RSV. Preterm = 1 day (IQR = 0 to 3) No difference Term = 1 day (IQR = 0 to 3) We calculated bronchiolitis hospital admission rates among term and preterm born infants. We also examined age at bronchiolitis admission and the median length of stay for admissions, as a proxy measure of severity of illness. Conclusions 85% of infants admitted to hospital with bronchiolitis in England are born at term and many are admitted for just 1 day. The peak in RSV bronchiolitis admissions at age 1 month is earlier than previously reported in other developed countries. These findings have important implications for both active and passive immunisation policies. Acknowledgements References We wish to thank the National Institute for Health Research (NIHR) “Medicines for Neonates” Programme Grant for Applied Research which provided the main source of funding for this study (Principal Investigator Professor Neena Modi, Imperial College London). We also thank Dr Paul Aylin and the Dr Foster Unit at Imperial College London for providing access to the Hospital Episode Statistics database. 1. Papadopoulos NG, Moustaki M, Tsolia M, Bossios A, Astra E, Prezerakou A et al. Association of Rhinovirus Infection with Increased Disease Severity in Acute Bronchiolitis. Am J Respir Crit Care Med 2002; 165(9):1285-1289. 2. Smyth RL, Openshaw PJ. Bronchiolitis. The Lancet 2006; 368(9532):312-322. 3. Hall CB, Weinberg GA, Iwane MK, Blumkin AK, Edwards KM, Staat MA et al. The Burden of Respiratory Syncytial Virus Infection in Young Children. The New England Journal of Medicine 2009; 360(6):588-598. 4. Hall CB. Respiratory syncytial virus in young children. The Lancet 2010; 375(9725):1500-1502. 5. Office for National Statistics. News Release: 1 in 13 live births in England and Wales are born preterm. http://www.statistics.gov.uk/pdfdir/preterm0507.pdf This publication presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0707-10010). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The funders had no role in the study design, collection, analysis, and interpretation of data, in the writing of the report or in the decision to submit the paper for publication. Email address: joanna.murray@imperial.ac.uk