2008-May 23- Grant Proposal (SC,TL) FINAL
advertisement
 FINAL")
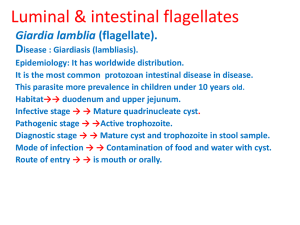
Chen, Samuel Lew, Thomas HumBio 153: Parasites and Pestilence Spring 2008 Grant Proposal Proposed Project: Improved examination of local epidemiology of Giardia infection and associated risk factors through Enzyme Immunoassay (EIA) technique in Mexico City Introduction: Giardia intestinalis, also known as Giardia lamblia and Giardia duodenalis, is one of the most common intestinal parasites in the world, causing the diarrheal illness named Giardiasis. G. intestinalis is a parasite that lives in the intestine and is passed in the stool, found worldwide and periodically in every region in the United States. The threat of morbidity is particularly potent in developing countries with poor water sanitation, where there are often high prevalence rates. While there are a disproportionate number of people affected by Giardiasis in the developing world, the most efficacious diagnostic and treatment tools are finding it difficult to reach these areas. Thus, a concerted effort must be made to determine true prevalence and incidence rates of Giardiasis in these areas with the most sensitive and efficient diagnostic tools. It will also be important to identify the regional risk factors associated with the disease occurrence. With this knowledge, public health officials will be better equipped to monitor and regulate the incidence and spread of Giardia infection in their populations. Specific Aims: This project will determine the vital current statistic of incidence of Giardia infection in Mexico City, as well as determine the risk factors associated with the disease that is present in this locale. 1 Particularly, we will aim to: 1) Use EIA to assess the incidence of Giardiasis in Mexico City -Pathology samples from all patients presenting with diarrheal disease will be obtained from a diverse group of public and private hospitals serving a representative subset of the population in Mexico City over 10 months. Stool samples will then assessed for Giardia infection using EIA. 2) Determine the risk factors present for Giardiasis in Mexico City -Patients presenting with diarrheal illness will be provided with a detailed survey regarding exposure to known risk factors for Giardia infection, as well as for socioeconomic status and familial information. - Giardia incidence will then be correlated with patient information to determine a ranked list of risk factors for Giardiasis spread in Mexico City. Incidence will also be examined for significant correlation with any of the risk factors. Background: Giardia lamblia, the intestinal parasite at the root of the disease Giardiasis, is the most highly diagnosed parasitic infection in the United States and other developed nations. In such industrialized nations, prevalence rates range from 2-7%. However, it is the developing world that carries the highest burden of this disease, with an average reported prevalence rate of 2030% (Furness 2000). In areas of particularly poor sanitation and water quality, such as parts of Mexico and Russia, this number can be as high as 95% (Ortega 1997). The problems associated with this parasite are not only characterized by their high prevalence, but also their potentially debilitating nature. 2 While Giardia infection is often asymptomatic, Giardiasis can also manifest itself through explosive diarrhea, flatulence, anorexia, abdominal pains, malabsorption, and vomiting. Infection can cause mortality in young children and those who are immunocompromised, contributing to the 1.8 million lives lost worldwide due to diarrheal diseases each year. Death in infants from Giardia and other diarrheal diseases are due to dehydration. This is the leading cause of death from infectious diseases globally in infants. Thus, in terms of morbidity and DALYs lost as a result of Giardia infection, Giardiasis remains an important infectious disease to consider. Diarrheal diseases alone account for 4.1%, or well over Figure 1 Life Cycle of Giardia, with focus on Human effects (Silva, et al) 40 million, of the global burden of total DALYs lost (WHO 2008). Giardia lamblia is a flagellated enteric protozoan parasite. There are two forms in the parasite life cycle (Figure 1): an infectious cyst form that is the parasitic stage that is passed into the environment through defecation, and a trophozoite stage, which is found within the infected organism (Silva 2007, John 2006). After ingestion of the cyst by a host, trophozoites are released into the intestine in a process known as excystation (Jones 1988). The trophozoite form attaches to the small intestine of the host via a sucking disk on the ventral surface. Easily recognizable, the trophozoite is a bilaterally symmetrical, di-nucleic tear-drop shape (Figure 2) (Qeli 2002). 3 While the mechanism of disease manifestation from Giardia infection is unclear, there are several competing theories regarding pathogenesis. These include protozoan damage to mucosa and villi structures, disturbance of the natural flora, and increased intestinal permeability via localized cytokine production (Smith 2008). These hypotheses are further supported by studies demonstrating that infected patients who remain asymptomatic exhibit minimal to non-existent damage in their small intestine (Farthing 1996). While the trophozoite form cannot survive in the environment, the cyst form remains infectious when passed through the feces. This hardy form of the protozoan can survive in cool, moist conditions for several months and can even withstand standard chlorine Figure 2 Trophozoite form of Giardia lamblia. Bi-lateral symmetric di-nculeic tear-drop shapes characterize the trophozoite stage. (Queli, Albi) treatment of water (Jones 1988). Transmitted in a fecal-oral manner, the cyst can infect a variety of reservoir hosts, including muskrats, cats, dogs, birds, cows, and beavers, hence the colloquial name “beaver fever”. Giardia lamblia can also become a widespread contaminant of foods, but is most commonly transmitted to humans as a waterbourne infectious disease in fecally contaminated groundwater finding its way into drinking water. Thus, in places such as Mexico City, where water sanitation can be a problem in and around a highly populated, urban area, the incidence can rise very quickly once a few people are infected. In fact, poor water quality, caused by such 4 things as contaminated groundwater sources, overcrowding, and poor sanitation in Mexico City, have contributed to an estimated consistent prevalence of 10% Giardia infection in many subpopulations (Cifuentes 2004). The metropolis is an ideal setting for interventions in education and sanitation efforts, in addition to mass treatment if accurate incidence and prevalence rates can be achieved. Diagnosis of Giardia infection, as it currently stands, is carried out in a variety of ways depending on the availability of materials. One traditional way of diagnosis is the identification of cysts in stool samples under the microscope, using the trichome stain or iron hematoxylin staining. An additional method that has been used widely in the past is the “string test,” in which a patient swallows a capsule with a string attached. The capsule passes through the small intestine where trophozoites attach to the string. The string is then pulled out and examined under the microscope for the presence of trophozoites. Microscopy of a duodenal biopsy is a third diagnostic technique that has been useful for identification of Giardia cysts and trophozoites. However, each of these methods depends on the eye to distinguish cysts and trophozoites from a sample, which can prove to be variable and, at times, unreliable. A more reliable test that has become highly accessible in the developed world is the enzyme-linked immunoassay, or commercialized EIA test (Figure 3), which detects Giardia antigens in the stool. Studies have shown that EIA testing is far more effective in determining Fig 3 Giardia EIA test kit from TechLab ® (TechLab, Inc) positive infection, as compared to standard staining-microscopy techniques (Srijan 2005). 5 Particularly, EIA testing was shown to be nearly two times more sensitive than sample examination, while remaining quicker and more economical than the conventional examination methods (Aziz 2001). Further, due to extreme variability with which the parasite is excreted in both symptomatic and asymptomatic infections, a single fecal examination may detect as few as 34% of Giardia infections. In comparison, the EIA test will detect a Giardia specific antigen when the patient is infected, whether or not the stool sample exhibits cysts or trophozoites (Marti 1993). Improved sensitivity of diagnostic tests for Giardiasis is of great importance, not only to shape public policy from accurate information on incidence and prevalence in a given area, but also to quickly and accurately diagnose the infection so that the patient can be effectively treated and endures the minimal amount of discomfort. It is also the most economic option for a population to rapidly and efficiently diagnose, since the infection can be treated easily and effectively with metronidazole and tinidazole, easing the burden of sick days. Both pharmaceutical products are nitroimidazoles that work against trophozoites, while tinidazole also acts against cysts in the body (Krishnamurthy 1978). Though treatment is easy, this intervention cannot feasibly happen without proper epidemiology. According to Odoi et al, little has been done in terms of geographic mapping of Giardiasis (Odoi 2003). The parasite wreaks havoc around the world, however the authors identify a tremendous lack of data on where Giardia infection is most prevalent and is least treated. In order for efficient intervention to relieve the burden of Giardiasis, accurate epidemiologic data must exist. In order for accurate epidemiology to exist, there must be efficacious diagnoses, and the most sensitive and specific assay is the EIA for the fecal antigen of Giardia cysts. 6 Accurate data detailing incidence and prevalence of Giardiasis can also be used to correlate with other factors that can serve as targets for intervention. Risk factors are diverse and great in number for Giardia infection. In Mexico City, significant risk factors that are currently known include close contact by schoolchildren, low standards of personal hygiene, unsafe methods of drinking water storage and food-related practices at the household level (Cifuentes 2004). Yet, behavioral risk factors may also play a role and geographic areas may be particularly susceptible to infection. These factors would therefore benefit from further investigation. Thus, by identifying these risk factors with efficacious surveying and ascertaining the true incidence of Giardiasis via EIA diagnostic techniques, we can identify the most efficient way to relieve Mexico City of this great burden. If we know the true epidemiological numbers regarding this largely waterborne illness, interventions to implement water treatment facilities or distribute metronidazole or tinidazole can be undertaken more successfully to the areas and populations most affected. 7 Study Design: Study Setting: Mexico City Mexico City was picked as an ideal location for this study due to the prevalence suggested by the lower standard of sanitation, poor water quality, and high density population. It is also at the heart of Mexico, which is considered a developing country. Study Subjects: Over a ten month period, all patients presenting with diarrheal diseases from a diverse group of hospitals and clinics in Mexico City will be assessed for Giardia infection through EIA test of their stool samples. Based on estimated data, approximately 1000 patients can then be recruited for the study. Those who return positive tests for Giardia will then be surveyed for risk factors. Assuming 75% retention, number of surveys requested should suffice for adequate power in statistical analysis. Study Design: 1) Use EIA to assess the incidence of Giardiasis in Mexico City: Select hospitals and clinics, serving representative samples of the population of Mexico City, will be requested to report all cases of diarrheal diseases to the investigation team. Upon presentation of diarrheal symptoms, physicians and healthcare personnel will be requested to acquire stool samples for pathological study. Approximately three grams of these fecal samples will be taken, labeled (i.e., identification, age, location), and transported at the end of the day to the investigation team’s laboratory. Samples will then be tested through provided EIA test kits for Giardia antigens. Number of positive Giardia diagnoses over time will be extrapolated to 8 the entire population to assess incidence rates. In a city populated by greater than 19 million people, acquiring 1000 samples over 10 months is a feasible goal. 2) Determine the role of risk factors present for Giardia infection in Mexico City: Of the patient population presenting with diarrheal illnesses and being tested via EIA of stool samples for Giardia infection, all individuals will be requested to fill out and return standardized surveys. The questionnaires will ask about socioeconomic status, exposure to potentially contaminated groundwater, sources of food, exposure to schoolchildren, and exposure to animal reservoirs, such as beavers, cows, deer, cats, dogs, birds and sheep. Surveys will be given out with approval of Institutional Review Boards and patients’ consent to participate in the study. Risk factors will then be ranked by percentage of diagnosed patients admitting to exposure. Data/Statistical Analysis: We expect from the approximately 1000 surveys distributed, approximately 75% will be returned completely filled out and eligible from accurate diagnosis. From the surveys of infected individuals, numbers of admissions to exposures to risk factors and levels of socioeconomic status will be tabulated. Results will then be ranked and evaluated using crude odds ratios with computed confidence intervals and relative risk calculations. Further examination will involve conditional logistic regression to estimate more precise odds ratios and confidence intervals and assess relative risk for Giardia infection with exposure to any of the risk factors, considering the variables presented in this study. Additionally, subgroups will be divided by sex, age and 9 socioeconomic status, for secondary evaluation to determine any significant conclusions regarding environmental, demographic or socioeconomic factors and their impact on Giardia infection incidence. 10 References 1. Furness BW, Beach MJ, Roberts JM. “Giardiasis surveillance--United States, 1992-1997.” MMWR CDC Surveill Summ. 2000 Aug 11;49(7):1-13. 2. Ortega YR, Adam RD. “Giardia: overview and update.” Clinical Infectious Diseases. 1997. 25(3):545-549 3. “Global Burden of Disease.” World Health Organization. May 15, 2008. http://www.who.int/topics/global_burden_of_disease/en/ 4. Silva, AJ, Moser M. “An illustration of The life cycle of Giardia Lamblia” National Institute of Health: National Institute of Allergy and Infectious Diseases. Sept. 19, 2007. May 15, 2008. 5. John DT, Petri WA. Medical Parasitology: 9th Edition. Saunders Elsevier: St Louis, MO. 2006 6. Jones JE. “Giardiasis.” Laboratory diagnosis of infectious disease, vol. 1 Springer-Verlag, New York. 1988:872-882. 7. Smith, D. Scott. “Lumen-Dwelling Protozoa.” Lecture. April 18, 2008. 8. Farthing MJ. “Giardiasis” Gastroenterol Clin North Am. 1996. 25(3):493-515. 9. Cifuentes E, et al. Risk of Giardia Intestinalis infection in children from an artificially recharged ground water area in Mexico City. Am J Trop Med Hyg, 2004. 71(2): 65 - 70. 10. Srijan A, Wongstitwilairoong B, Pitarangsi C, Serichantalergs O, Fukuda CD, Bodhidatta L, Mason CJ. “Re-evaluation of commercially available enzyme linked immunosorbent assay for the detection of Giardia lamblia and Cryptosporidium spp from stool specimens” Southeast Asian J Trop Med Public Health. 2005. 36(1):26-29 11. Aziz H, Beck CE, Lux MF, Hudson MJ. “A comparison study of different methods used in the detection of Giardia lamblia” Clinical Laboratory Science 2001 14(3):150-154 12. Marti H, Koella JC. “Multiple stool examinations for ova and parasites and rate of falsenegative results. J Clin Microbiology. 1993 31(22): 3044-3045 13. Krishnamurthy KA, Saradhambal V. “Single dose therapy of giardiasis: a comparative study of tinidazole and metronidazole in pediatric patients” Indian Pediatr. 1978 Jan;15(1):51-6. 14.. Odoi et al. “Geographical and temporal distribution of human giardiasis in Ontario, Canada.” International Journal of Health Geographics. 2003 2(5): 115-128 11 Figure References: 1. Silva, AJ, Moser M. “An illustration of The life cycle of Giardia Lamblia” National Institute of Health: National Institute of Allergy and Infectious Diseases. Sept. 19, 2007. May 15, 2008. 2. Qeli, Albi. Accessed May 14, 2008. http://www.argjiro.net/albi/white/meded/?book=2&chapter=0&subchapter=0 3) TechLab. “PT5012 - GIARDIA II.” 2001. Accessed May 17, 2008 http://www.techlab.com/product_details/pt5012.htm 12