Temporal bone fracture and its complication
Mar. 6th, 2002. 整理者: R3 邱贊仁
Temporal bone fracture (TBF):
1. Clinical criteria:
head trauma history, PE: otorrhea, hemotympanum, facial nerve paralysis.
2. Clinical and radiological criteria:
head trauma history, PE, HRCT.
*Although HRCT has improved the radiological diagnosis of temporal bone fractures,
the diagnosis must often be based on clinical findings alone4.
Incidence of TBF:
30~75% blunt head trauma1
14~22% skull fracture2
2% head-injured patients6
Etiology of TBF:
Motor vehicle accidents2, assult, fall, motorcycle, pedestrian…
Children1:
0~4 y/o: falls
4~14 y/o: Motor vehicle accidents
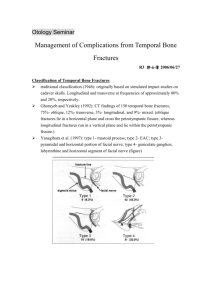
TBF classification: (arbitrary)
1. The fracture line relative to the long axis of the petrous bone.
Longitudinal: parallel
Transverse: perpendicular
mixed
Longitudinal
Transverse
long axis of petrous
parallel
perpendicular
frequency
most common, 70~90%
20~30%
external ear canal laceration frequent, bleeding
middle ear bleeding
ossicles disruption
frequent, hemotympanum
common, CHL
otic capsule involve
common, SNHL
vestibular involve
mild, concussive effect
facial paralysis
10~25%2, often delay onset 30~50%2, immediately
CSF leak
may be loss, concussive or
otic capsule fracture
Traumaedema
facial n interruption
less common
common
2. Yanagihara N3 (3 D helical CT): type 1, 2, 3, 4 (4a, 4b) surgical & radiological
significance.
Evaluation:
Head injury patients presented to the emergency room
@ABC principles(maintain respiratory & circulatory function): first
@Evaluate neurologic status
@Facial n function evaluation: (initial facial n evaluation is very important)2,4
(conscious vs unconscious pts---stimulating paingrimace)
@ear, EAC, tympanic membrane(TM) evaluation:
EAC laceration, bony fracture
TM perforation: location, shape(slit, triangular, stellate)
Ear bleeding: D/D from EAC lacerated skin or middle ear active bleeding
@middle ear active bleeding: possible CSF leakage
*How to manage the ear bleeding (ear canal packing or not)?
*How to diagnose CSF otorrhea or rhinorrhea?
@Vestibular system evaluation: Nystagmus (important)
Nystagmus:
Direction change or vertical nystagmus: central injury
Destructive lesion: toward the noninvolved side
Irritative lesion: toward the involved side
@Audiologic evaluation: Weber test(Tunning fork) at ER
PTA, speech discrimination, acoustic reflex
@Radiologic evaluation:
Potential skull base fracture: HRCT of temporal bone (s contrast)
HRCT: 1.5~2.0mm thickness, axial view, coronal view if possible.
Complication:
1. TM traumatic perforation & external auditory canal stenosis
Remove blood clot from the EAC by suction gently.
EAC laceration: severestented with a pack to prevent stenosis
Fracture-dislocation of EAC: reduction by Killian nasal speculum and EAC pack
Initial relocation the fracture-dislocation of EAC is beneficial and important.
Scarstenosis difficult to correct
TM perforation:
Slit-like P: spontaneous healing
Triangular or stellate P: (big P size)
Small-angled pickgently tease this flap back into its anatomic position
Transcanal paper myringoplasty
Otics is not suggested for dry, clean, traumatic TM perforation.
2. CSF otorrhea, rhinorrhea, otorhinorrhea (potential meningitis2):
Incidence: 26% TBF4
Diagnosis1:
(1) PE(serosanguineous drainage from the ear or nose)
(2) History of antecedent temporal bone trauma
(3) Determination of the fluid as CSF
How to determine the otorrhea/rhinorrhea as CSF?
(1) Filter paper: halo sign or double ring. (highly suggestive)
(2) β-2 transferrin(100% sensitivity, 95% specificity)5:
a protein found in CSF and perilymph
not in blood, nasal secretion,or middle ear secretion.
advantages: small sample size for analysis(<1 mL)
resistance to contamination by other fluids
require no special handling or refrigeration
(3) Glucose content test(biochemical): unreliable
False positive rate:45~75%
(4) Sugar dipstick: unreliable, particular in the presence of blood
(5) Nuclear medicine evaluation: intrathecal injection of
fluorescein or a radioactive carrier substance
Management:
Medical (conservative) approach: no other intracranial injury.
>90% resolve spontaneously(7~10days)1,2.
(1) bed rest
(2) head of bed elevation
(3) avoid of straining: constipation, coughing, nose blowing
(stool softener, anti-tussive, anti-histamine)
(4) lumbar drain: decrease CSF pressure
Surgical repair:(indication)
(1) CSF leak persists for 7~10 days (meningitis chance)2
(2)A large petrous bone defect1
(3)Late onset CSF leak1
(4)Brain herniation1
(5)Recurrent episodes of meningitis1
*Antibiotic prophylaxis: necessary? Is it beneficial in reducing post-traumatic
meningitis?
Canniff et al9: 1800 head injury, CSF otorrhea 1.4%, 20%meningitis
(1) increased risk of developing meningitis2: CSF leak>7days, concurrent infection
(2) benefit: Brodie et al2 (CSF fistula present)
(3) not benefit: Hoff et al2, Lee et al1, inadequate management and affect culture
results9
(4) adequate prophylaxis Abx9: broad-spectrum Abx and cross BBB
3. Facial paralysis:
Incidence1:
before CT use: 11%
recent:3~4%
Evaluation:
(1) House-Brackmann grading system(I~VI)
DEFS
(2) Topographic diagnosis: simple & definitive. Great discrepancy
Schirmer tear test
Acoustic (stapedial reflex)
Taste tests
Salivary tests
(3) Electrical tests: reliability be challenged
Evaluate the physiologic extent of n damage
Predict prognosis, determine treatment.
Many times exams: D/D degeneration/regeneration
Maximal nerve excitability test(MST)
Electroneurography/Evoked electromyography(EnoG)
Electromyography(EMG)
Onset: immediate vs delay onset (initial evaluationvery important)
Immediate onset: severed facial n chance
delay onset: traumaedematous process
Surgical intervention vs Medical management
Surgical intervention
Medical management
Onset
immediate
delay
severity
complete
incomplete
ENoG
>=90%, Fisch et al.
<90%
Fracture type
transverse
longitudinal
Medical management: steroid, careful facial n monitoring
Surgical management:
The key factor in the decision to decompress is whether a severed nerve is suspected.
Barrs et al4: empty axonal tubules 5 days after trauma, nearly complete at 21 days
Animal study: for crushed or severed facial nretrograde degeneration within 30
days. Regeneration was prevented.
Most common site for facial n injury:
(1) Distal labyrinthine segment near the geniculate ganglion8
(perigeniculate region)
(2)Mastoid segment(distal to the second genu)
Facial nerve exploration and decompression
For n repair, release edemaprevent fibrosis, scarringregeneration
Severe n degeneration
Fisch
Lambert & Brackmann
Transection n.
30%
23%
Bony impingement
20%
38%
Intraneural hematoma
50%
8%
Localized swelling
0
31%
(1) transmastoid supralabyrinthine approach
(2) translabyrinthine approach: total loss of auditory & vestibular function
(3) middle fossa approach
(4) combined transmastoid and middle fossa approach: for preserved hearing
Conclusion(Summary)
1. Facial n function initial evaluation at ER is very important.
Delayed onset of facial paralysis, surgical decompression is rarely indicated.
2. CSF fistula generally close spontaneously with conservative management
within 1 week.
3. Increased risk of developing meningitis: CSF fistula>7 days, concurrent
infection.
4. Prophylactic antibiotics: controversial
CSF fistula present: use2
Broad spectrum and cross BBB9.
Detailed method for facial n decompression: discussion at next section
References:
1. Lee D, Honrado C, Har-El G, et al. Pediatric temporal bone fractures.
Laryngoscope 1998;108:816-21.
2. Brodie HA, Thompson TC. Management of complications from 820 temporal
bone fractures. Am J Otol 1997;18(2):188-97
3. Yanagihara N, Murakami S, Nishihara S. Temporal bone fractures inducing facial
nerve paralysis: A new classification and its clinical significance. ENT J 1997;
76(2):79-86
4. Nageris B, Hansen MC, Lavelle WG, et al. Temporal bone fractures. Am J Emerg
5.
6.
7.
8.
9.
Med 1995;13(2):211-4.
McGuirt WF, Stool SE. Cerebrospinal fluid fistula: the identification and
management in pediatric temporal bone fractures. Laryngoscope 1995;105:359-64
Eby TL, Pollak A, Fisch U. Intratemporal facial nerve anastomosis: A temporal
bone study. Laryngoscope 1990;100:623-6.
Ylikoski J. Facial palsy after temporal bone fracture: light and electron
microscopic findings in two cases. J Laryngo Otol 1988;102:298-303.
Eby TL, Pollak A, Fisch U. Histopathology of the facial nerve after longitudinal
temporal bone fracture. Laryngoscope 1988;98:717-20.
Kinney SE. Trauma to the middle ear and temporal bone. Otolaryngology head
and neck surgery. Mosby, 1998;3076-87.
10. Dobie RA. Tests of facial nerve function. Otolaryngology head and neck surgery.
Mosby, 1998;2757-66.
 0
0