National Pathology Programme
Standardisation and
Harmonisation
Gifford Batstone
National Pathology Programme
© The Strategic Projects Team
Hosted by the Greater East Midlands Commissioning Support
Unit
April TRUD Release
• Revised list of units of measurement
• PBCL and NLMC
• New entries – 294
• Inclusion of sample type
• Corrections to names eg BNP
• Deletions – 299
• Duplications
• Linked to corrections
© The Strategic Projects Team
Hosted by the Greater East Midlands Commissioning Support
Unit
Supplementary File
• Guidance at present/mandatory in future
• Linking analytes (with analysed specimen
type) to a single unit of measurement
• Addition of Data Combination Indicators
•
•
•
•
•
0 = test not used to trend
1 = OK to assume combination
2 = requires a factor
3 = don’t even think about it
4 = not yet agreed
© The Strategic Projects Team
Hosted by the Greater East Midlands Commissioning Support
Unit
Why? - PQAR
‘The continued development of the NLMC to
ensure consistency of data and information
across the NHS in England should remain a
priority. The professional bodies, the IVD
manufacturers and others should work towards
minimising the differences between analytical
processes, requesting and reporting.’
Recommendation 4.66 Pathology Quality Assurance Review
Why? - PQAR
‘Laboratory processes should be harmonised so
that patients can be confident about the
consistency of their test results, especially as
they start to gain access to their personal health
records that may contain reports from different
pathology services’
Press Release, Pathology Quality Assurance Review
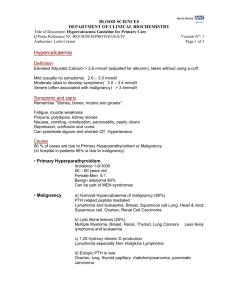
Ref Range Variation
• Self reported reference
intervals for TSH and fT4.
• Each bar represents a
different laboratory
• Each colour represents a
single analytical method
• Statistical analysis
750,000 TSH reports gives
0.5 - 5.5 mU/L but
?variation - age, method
• Data Finlay MacKenzie
UKNEQAS 09/2012
© The Strategic Projects Team
Hosted by the Greater East Midlands Commissioning Support
Unit
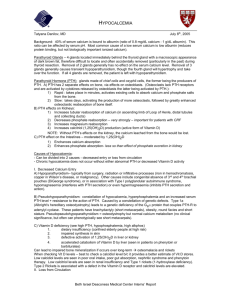
TSH values:
Geometric Mean
before (A) and
after (B)
mathematical
recalibration
16 immunoassays
from 9 different
manufacturers
analysing the same
sample in
triplicate.
Report of the IFCC Working
Group for Standardization
of Thyroid Function Tests;
Part 1: Thyroid-Stimulating
Hormone
Thienpont L et al; Clinical
Chemistry 56:6 902–911
(2010)
Serum Albumin Variation – Age
and Sex
Gary Weaving et al
46
male
albumin (g/L)
45
44
43
female
42
41
40
39
38
10
80 - 90
70 - 80
8
60 - 70
50 - 60
6
40 - 50
30 - 40
4
20 - 30
2
Age group
© The Strategic Projects Team
Hosted by the Greater East Midlands Commissioning Support
Unit
Average Albumin by laboratory
50
male
48
48
46
46
44
44
42
42
40
40
38
38
36
36
34
34
32
32
30
female
age group
© The Strategic Projects Team
7
8
9
80 - 90
6
70 - 80
5
60 - 70
4
50 - 60
3
40 - 50
2
30 - 40
10
20 - 30
80 - 90
8
70 - 80
6
50 - 60
40 - 50
30 - 40
4
60 - 70
30
2
20 - 30
albumin (g/L)
50
10
age group
Hosted by the Greater East Midlands Commissioning Support
Unit
Effect of assay on dose
Mike Bosomworth
Method Mean Creatinine
(μmol/l)
Enzymatic
50
Kinetic Jaffe
64
Jaffe - Compensated
60
O'Leary
67
Endpoint Jaffe
68
IDMS Value
50
Variability
34%
© The Strategic Projects Team
Female, 45y, 55kg
C&G
Carboplatin
(ml/min)
(mg)
108.5
801
85.4
663
90.8
695
81.2
637
80.8
635
109.2
805
34%
26%
Hosted by the Greater East Midlands Commissioning Support
Unit
Comparison of 5 PTH methods
Mean values of NEQAS distributions of
Synthetic PTH - Sanjay Khanna
Reference
Ranges
1.17- 9.22
1.59 - 7.27
1.48 - 7.63
1.27 - 9.33
1.59 - 6.89
Taking PTH results from 1735 CKD 5 patients in
Brighton; Data transformed from Roche to other
analytical methods and UKRA ULN applied
No. of CKD stage 5 patients
1800
1600
490
499
>9xULN
(HTBD)
364
526
478
1400
1200
<2xULN
(LTBD)
1000
891
800
830
869
415
367
890
887
600
400
200
0
2-9xULN
(optimal)
480
319
370
Traceability Categories from ISO 17511
Standardization
Category
Reference
measurement
procedure
Primary (pure
substance)
reference
material
Secondary
(value
assigned)
reference
material
Examples
1
Yes
Yes
Possible
Electrolytes,
glucose,
cortisol
2
Yes
No
Possible
Enzymes
3
Yes
No
No
Hemostatic
factors
4
No
No
Yes
Proteins,
tumor markers,
HIV
5
No
No
No
Proteins,
EBV, VZV
Harmonization
Miller 2012
Standardisation of Reports
The emphasis is on the reports
More than one approach:
• Standardisation of analytical techniques
• Use of WHO and similar reference materials
• Mathematical alignment of methods
– Mean values of different methods
• Where no international reference materials
– To WHO reference based methods
Questions and Comments
please
Same labs Adj Calcium Females
average total calcium
average adjusted calcium
2.55
2.50
2.45
2.45
2.40
2.40
calcium (mmol/L)
2.50
2.35
2.30
2.25
2.35
2.30
2.25
2.20
2.20
2.15
2.15
2.10
5
6
7
age group
8
9
80 - 90
4
70 - 80
3
60 - 70
2
50 - 60
10
40 - 50
9
30 - 40
60 - 70
age group
8
20 - 30
7
80 - 90
6
70 - 80
5
50 - 60
4
40 - 50
3
30 - 40
2.10
2
20 - 30
calcium (mmol/L)
2.55
10
Effect of adj to age related alb
calcium adjusted by lab
calcium re-adjusted for age differences
in albumin
mean +/- 2sd
mean +/- 2sd
80 - 90
70 - 80
60 - 70
50 - 60
40 - 50
30 - 40
20 - 30
30
22
80 - 90
70 - 80 28
60 - 70
50 - 60 26
40 - 50
30 - 40 24
20 - 30
20
20
28
female
80 - 90
70 - 80
60 - 70
50 - 60
40 - 50
30 - 40
20 - 30
26
24
22
18
male
male
female
30
16
14
12
12
10
1.8
80 - 90
70 - 80 18
60 - 70
50 - 60 16
40 - 50
30 - 40 14
20 - 30
10
1.9
2.0
2.1
2.2
2.3
2.4
calcium (mmol/L)
2.5
2.6
2.7
2.8
1.8
1.9
2.0
2.1
2.2
2.3
2.4
2.5
calcium (mmol/L)
2.6
2.7
2.8
Comparison of range of results produced with laboratory reference range
Females
age 20 – 30 yr
3.0
reference range
width
2.0
1.0
0.0
-1.0
-2.0
-3.0
Spread of results vs mean of results
3.0
acceptable?
> 10 %
2.0
1.5
1 – 10 %
1.0
0.1 – 10 %
0.5
0 – 0.1 %
mean
-1.5
-1.0
-0.5
0.0
% results lower than reference range
0.5
1.0
<1 %
-2.0
1 – 10 %
-2.5
10 – 20 %
-3.0
20 - 40 %
0.0
< 40 %
% results lower than reference range
2.5
F, age 20 -30
spread
Adjusted Calcium