Chronic myeloid leukaemia
David Marin,
Imperial College London
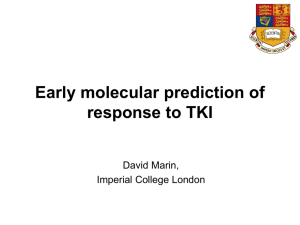
Survival of 246 patients who received Interferon therapy within the
UK Medical Research Council's CML-III trial (1986-1994)
1.0
Survival of 224 patients
who received first line
imatinib therapy therapy in
Hammersmith
Hospital
(2000-2008)
.9
.8
Survival
.7
.6
.5
.4
.3
.2
.1
0.0
0
2
4
6
8
10
12
14
Time from diagnosis (years)
16
18
20
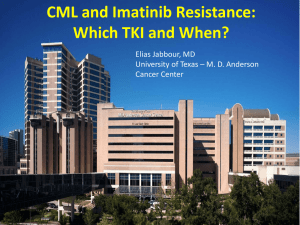
28 May 2001
2001
Imatinib mesylate (STI571 - Glivec)
(C30H35N7SO4)
H
N
N
N
N
H
N
N
N
N
O
1998
(From Novartis Pharma)
Mechanism of action of imatinib
Bcr-Abl
Bcr-Abl
Substrate
Substrate
P
P
P
Y
ATP
Imatinib
P
Y = Tyrosine
P = Phosphate
Bosutinib
(SK-606)
Ponatinib
Target kinases for the 4 TKIs
Selectivity of Tyrosine Kinase Inhibitors
Imatinib
(Phos. IC50)
PDGFR
72 nM
Nilotinib
(Phos. IC50)
BcrAbl
20 nM
Dasatinib
(Phos. IC50)
Src
0.1 nM
Bosutinib
(Phos. IC50)
Src
3 nM
>
Kit
99 nM
>
PDGFR
75 nM
>
BcrAbl
1.8 nM
>
BcrAbl
85 nM
>
BcrAbl
221 nM
>
Kit
209 nM
>
PDGFR
2.9 nM
>
PDGFR
>3000
1. Manley PW, et al. Proc Am Assoc Cancer Res 2007;48:772.
2. Weisberg E, et al. Cancer Cell 2005;7:1129.
3. Remsing Rix LL, et al. Leukemia 2009;23:477.
>
Src
>1000 nM
>
Src
>1000 nM
>
Kit
18 nM
>
Kit
>10000 nM
Comparison of Kinase Inhibitors: Toxicity
Imatinib
(STI571)
Gleevec*
Nilotinib
Dasatinib
(AMN 107) (BMS354825)
Tasigna*
Sprycel*
Bosutinib
(SK606)
Hematologic
++
++
++
+
Pleural Effusions
-
-
+++
+
Hepatic
+
++
+
+
Pancreatitis
-
+
-
-
GI Bleeding
-
-
++
-
Platelet Function
-
-
+
?
Immune
-
-
++
?
Diarrhea
+
+
+
+++
Q-Tc
-
++
++
+?
Licensed
First Line
Second Line
Imatinib
1st and 2nd line
Gold standard
No published
experience
Nilotinib
1st and 2nd line
Early data suggest
small advantage
over Imatinib
40-50% CCyR
Dasatinib
1st and 2nd line
Early data suggest
small advantage
over Imatinib
40-50% CCyR
Bosutinib
No (1st line soon)
Not yet clear,
maybe slightly
better than imatinib
40-50% CCyR
Ponatinib
No (2nd line soon?)
No yet tried
10-30% of
responses in 3rd line
(T315I active)
Darling, this
morning I
saw a new
patient with
CML and I
prescribed
him a TKI.
¿Darling,
Should not
you check
whether the
patient is
responding
?
I have done
my duty!
Patients who fail to achieve CCyR
progress to advance phase (n=204)
1.0
0.9
0.8
Probability of PFS
0.7
0.6
0.5
0.4
0.3
p<0.0001
0.2
0.1
0.0
0
6
12
18
24
30
36
42
48
54
60
Months from starting imatinib therapy
Marin, Blood 2008
Patients who achieve CCyR do well and patients who fail
to achieve CCyR do badly (IRIS data)
100
% without progression
90
p<0.001
80
70
60
50
40
Estimated rate (95% CI)
at 42 months:
30
20
10
CCyR
No CCyR
n=363
n=139
93% (89%, 96%)
74% (66%, 92%)
0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Months since randomization
TKI therapy only prolongs live on those patients who achieve CCyR
2G-TKI responders, n=67,
aRR=0.05, p=0.003
1.0
0.9
Imatinib responders, n= 179,
aRR= 0.18, p<0.0001
Provability of OS
0.8
0.7
0.6
0.5
Interferon controls, n =246,
aRR=1
0.4
0.3
0.2
0.1
0.0
0
1
2
3
4
5
6
7
TKI non responders, n= 37
aRR= 0.76, p=0.65
Time from diagnosis (years)
Ibrahim, Haematologica 2011
Patients must achieve CCyR
• How we know that the patient has
achieved CCyR?
• When the patient has to achieve CCyR?
• How we make sure that the patient
remains in CCyR?
Patients must achieve CCyR
• How we know that the patient has
achieved CCyR?
• When the patient has to achieve CCyR?
• How we make sure that the patient
remains in CCyR?
Patients must achieve CCyR
• How we know that the patient has
achieved CCyR?
• When the patient has to achieve CCyR?
• How we make sure that the patient
remains in CCyR?
100
10
10
Ph-chromosome pos
1
0.1
0.01
10
10
10
RT-PCR positive
(Ph-negative)
10
10
0.001
10
0.0001
10
10
10
RT-PCR negative
10
10
13
12
11
10
9
8
7
6
5
4
3
2
Total number of leukaemia cells
BCR-ABL/ABL ratio (%)
Leucocytosis
10
0
0
Adapted from Lin et al. Genes Chromosomes and Cancer 1995
Metaphases
Transcript
level at
diagnosis
100
1013
High WBC
Ph +
Metaphases
1012
BCR/ABL/ABL ratio (%)
Ph +
10
1
CHR
1011
1010
0.1
109
0.01
108
0.001
107
Total number of leukaemia cells
Normal WBC
PFS and probability of CCyR according to the
haematological response at 3 months
1.0
CHR, n=216
Probability of PFS
Cumulate incidence of CCyR
0.9
0.8
0.7
0.6
No CHR, n=8
0.5
0.4
0.3
PFS: p=0.002
0.2
CCyR: p=0.0003
0.1
0.0
0
6
12
18
24
30
36
42
48
54
60
Months from starting imatinib therapy
Marin, Blood 2008
Transcript
level at
diagnosis
Metaphases
CHR
Ph +
Metaphases
1012
Ph -
10
1
Ph +
MiCyR
1011
1010
0.1
109
0.01
108
0.001
107
Total number of leukaemia cells
BCR/ABL/ABL ratio (%)
100
1013
Transcript
level at
diagnosis
100
1013
Metaphases
Ph +
Ph -
MiCyR
Ph +
Metaphases
10
Ph +
MCyR
1
1011
Ph -
1010
0.1
109
0.01
108
0.001
107
Total number of leukaemia cells
MiCyR
BCR/ABL/ABL ratio (%)
1012
CHR
1013
Metaphases
100
Ph +
Ph Ph +
Ph +
10
MCyR
MCyR
1011
Ph -
Metaphases
1010
1
CCyR
Ph -
0.1
109
0.01
108
0.001
107
Total number of leukaemia cells
MiCyR
BCR/ABL/ABL ratio (%)
1012
CHR
1013
Metaphases
100
Ph +
Ph Ph +
Ph +
10
MCyR
1011
Ph -
Ph -
1
CCyR
1010
CCyR
Metaphases
109
0.1
MMR
Ph -
0.01
108
0.001
107
Total number of leukaemia cells
MiCyR
BCR/ABL/ABL ratio (%)
1012
CHR
1013
Metaphases
100
Ph +
Ph Ph +
Ph +
10
MCyR
1011
Ph -
Ph -
1
1010
CCyR
MMR
0.1
109
MMR
Ph -
108
0.01
Metaphases
0.001
CMR
107
Ph -
Total number of leukaemia cells
MiCyR
BCR/ABL/ABL ratio (%)
1012
CHR
Patients must achieve CCyR
• How we know that the patient has
achieved CCyR?
• When the patient has to achieve CCyR?
• How we make sure that the patient
remains in CCyR?
A, 3 months
1.0
1-35% Ph+
0.9
36-95% Ph+
0.8
0.7
0.6
0.5
0.4
96-100% Ph+
0.3
0.2
0.1
0.0
0
12
18
24
30
36
42
B, 6 months
1.0
48
54
Months from start of imatinib therapy
60
1-35% Ph+
0.9
36-95% Ph+
0.8
0.7
0.6
0.5
0.4
0.3
0.2
96-100% Ph+
0.1
p< 0.0001
6
Cumulative incidence of response
Cumulative incidence of response
Probability of CCyR according
to the cytogenetic response at 3 and 6 months (n=204)
0.0
0
p< 0.0001
6
12
18
24
30
36
42
48
54
Months from start of imatinib therapy
de Lavallade, JCO 2008
60
Patients must achieve CCyR
• How we know that the patient has
achieved CCyR?
• When the patient has to achieve CCyR?
• How we make sure that the patient
remains in CCyR?
How to monitor the patient and desired responses
G-Banding
{
•MiCyR?
•MCyR?
•CCyR?
{
•MMR?
•Early detection
of relapse
RQ-PCR
100
10
BCR/ABL/ABL ratio (%)
CCyR
1
3 log
0.1
FISH negative
0.01
0.001
Level of detection
0.0001
3
6
9
12
15
18
21
24
27
Months from start of imatinib
So, what is the
best first line
therapy?
ENESTnd: Nilotinib vs Imatinib in CML-CP
Study Design and Endpoints
• N = 846
• 217 centers
• 35 countries
R
A
N
D
O
M
I
Z
E
D
*
Nilotinib 300 mg BID (n = 282)
Nilotinib 400 mg BID (n = 281)
Imatinib 400 mg QD (n = 283)
Follow-up
5 years
• Primary endpoint:
• Key secondary endpoint:
• Other endpoints:
*Stratification by Sokal risk score
MMR at 12 months
Durable MMR at 24 months
CCyR by 12 months, time to MMR
and CCyR, EFS, PFS, time to AP/BC on
study treatment, OS including follow-up
30
Larson R. A. et al.JCO 28:7s ASCO 2010 (suppl; abs 6501, Oral)
Dasatinib Versus Imatinib Study In Treatmentnaïve CML: DASISION (CA180-056). Design
• N=519
• 108 centers
• 26 countries
Dasatinib 100 mg QD (n=259)
Follow-up
Randomized*
5 years
Imatinib 400 mg QD (n=260)
*Stratified by Hasford risk score
● Primary endpoint: Confirmed CCyR by 12 months
● Secondary/other endpoints: Rates of CCyR and MMR;
times to confirmed CCyR, CCyR and MMR; time in
confirmed CCyR and CCyR; PFS; overall survival
31
ASCO 2010, Abstract # LBA6500
ENESTnd: Nilotinib vs Imatinib in CML-CP
CCyR Rates* by 12 Months and Overall
Nilotinib 300 mg BID
Nilotinib 400 mg BID
Imatinib 400 mg QD
P < .001
P < .0001
100%
80%
80%
P = .017
P < .001
85%
78%
82%
74%
% CCyR
65%
60%
40%
20%
n = 282 n = 281
n = 283
n = 282
n = 281 n = 283
0%
Month 12
•
Overall
Among patients who had a cytogenetic assessment at 18 months
(n = 442/846), the rates of CCyR were:
•
99%, 99%, and 89% for nilotinib 300 mg BID, 400 mg BID, and imatinib
*ITT population
32
Data cut-off: 2Jan2010
Larson R. A. et al.JCO 28:7s ASCO 2010 (suppl; abs 6501, Oral)
DASISION: First-Line Dasatinib vs. Imatinib
in CML-CP. CCyR rates (ITT)
100
Dasatinib 100mg QD
80
CCyR
(%)
60
40
Imatinib 400mg QD
83
78
73
P=0.0011
67
72
59
54
31
20
0
Mo 3
•
33
Mo 6
Mo 9
Mo 12
By analysis of time to CCyR, likelihood of achieving CCyR at any
time ~50% higher with dasatinib than with imatinib (stratified
log-rank P<0.0001; HR=1.53)
ASCO 2010, Abstract # LBA6500
ENESTnd: Nilotinib vs Imatinib in CML-CP
Patient Disposition
Nilotinib
300 mg BID
Still on treatment
Discontinued, %
Disease progression*
Suboptimal response/
treatment failure*#
Adverse events
Abnormal lab. values
Death
Protocol violation
Other reason
Nilotinib
Imatinib
400 mg BID 400 mg QD
n = 282
80%
20
n = 281
81%
19
n = 283
75%
25
<1
<1
4
6
2
8
5
2
1
2
4
10
2
0
2
3
8
1
0
1
3
*Investigator assessment of criteria
#Patients
were required to discontinue nilotinib 300 mg BID for suboptimal response
Data cut-off: 2Jan2010
but could remain on nilotinib 400 mg BID
Larson R. A. et al.JCO 28:7s ASCO 2010 (suppl; abs 6501, Oral)
DASISION: First-Line Dasatinib vs. Imatinib
in CML-CP. Treatment Discontinuations
% Patients
Dasatinib 100 mg QD Imatinib 400 mg QD
n=258
n=258
Still on treatment
84.5
81.4
Discontinued
15.5
18.6
Treatment failure
including progression
5.0
8.9
Study drug toxicity
5.0
4.3
Adverse event unrelated
1.2
0.4
Other reason*
4.2
5.0
*Includes
35
consent withdrawal, pregnancy, lost to follow-up and death
ASCO 2010, Abstract # LBA6500
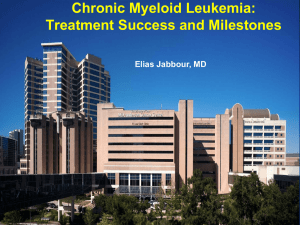
Outcome in 282 patients treated with imatinib
first line in Hammersmith Hospital
94%
6% death non CML
84%
10% death because the CML
77%
7% alive but not in CCyR
29% in CCyR but not on imatinib
48%
48% in CCyR on imatinib
Outcome in 135 patients treated with second line
dasatinib or nilotinib in Hammersmith Hospital
Probability
OS, 82%
C-CCyRS, 54%
EFS, 35%
Time (years) from the onset of second line therapy
Outcome in 135 patients treated with second line
dasatinib or nilotinib according to the cytogenetic
response achieved at 12 months
Probability of cCCyR-S
CCyR at 12 months, n=48
p=0.008
no CCyR at 12 months, n=51
Time (years) from the onset of second line therapy
Outcome in 135 patients treated with second line
dasatinib or nilotinib according to the cytogenetic
response achieved at 12 months
Probability
CCyR at 12 months, n=48
no CCyR at 12 months, n=51
Time (years) from the onset of second line therapy
It is far from certain which is going to be
the best line therapy as the log term
benefit of a modest improvement in the
CCyR rate induced by a given drug may
be easily overcome by a higher therapy
discontinuation rate on that drug
Cumulative incidence of CCyR in patients treated with
dasatinib first line therapy in the SPIRIT-II trial according to
the molecular response achieved at 3 months
Cumulative incidence of CCyR
3 months BCR-ABL/ABL <10%
3 months BCR-ABL/ABL >10%
p=0.02
Time from diagnosis (months)
Cumulative incidence of CCyR in the SPIRIT-II trial
according to the treatment arm and the molecular
response achieved at 3 months
Cumulative incidence of CCyR
3 months BCR-ABL/ABL <10%
3 months BCR-ABL/ABL >10%
Dasatinib
Imatinib
Time from diagnosis (months)
The key
principles of
therapy are:
1. Promptly identification of the
high risk patients
2. Change of therapy according to
tolerance and response
What is the best
why to detect
who is not doing
well?
A, 3 months
1.0
1-35% Ph+
0.9
36-95% Ph+
0.8
0.7
0.6
0.5
0.4
96-100% Ph+
0.3
0.2
0.1
0.0
0
12
18
24
30
36
42
B, 6 months
1.0
48
54
Months from start of imatinib therapy
60
1-35% Ph+
0.9
36-95% Ph+
0.8
0.7
0.6
0.5
0.4
0.3
0.2
96-100% Ph+
0.1
p< 0.0001
6
Cumulative incidence of response
Cumulative incidence of response
Probability of CCyR according
to the cytogenetic response at 3 and 6 months (n=204)
0.0
0
p< 0.0001
6
12
18
24
30
36
42
48
54
Months from start of imatinib therapy
de Lavallade, JCO 2008
60
We can do
better than
that!
We can identify what is the 3 months transcript level that predicts
for overall survival with the maximal sensitivity and specify
Survival in 282 patients treated with imatinib first line in
Hammersmith Hospital according to the molecular response
achieved at 3 months
Probability of survival
BCR-ABL/ABL<10% OS= 93.3%
BCR-ABL/ABL>10% OS= 54%
p<0.0001
Time from onset of imatinib therapy (years)
Outcome in 282 patients treated with imatinib first line in
Hammersmith Hospital according to the molecular response
achieved at 3 months
Probability of c-CCyRS
BCR-ABL/ABL<10%, c-CCyRS= 91%
BCR-ABL/ABL>10% c-CCyRS= 48%
p =0.0002
Time from onset of imatinib therapy (years)
Evolution of the transcript level in 282 patients treated
with imatinib first line therapy
Off
Imatinib
BCR-ABL1/ABL1 (log)
high transcript level at 3 month
CMR
low transcript level at 3 month
8-year cumulative incidence of CMR on imatinib therapy according
to the BCR-ABL1 transcript level at 3 months.
Cumulative incidence of CMR
3-month transcript ratio ≤0.61% (n=57), 8-year CI of CMR of 84.7%,
p<0.0001
3-month transcript ratio >0.61% (n=222), 8-years CI of CMR of 1.5%
Time from onset of therapy (years)
It is important to
achieve MMR?
Molecular responses
100
10
BCR/ABL/ABL ratio (%)
CCyR
1
3 log
0.1
FISH negative
0.01
0.001
Level of detection
0.0001
3
6
9
12
15
18
21
24
27
Months from start of imatinib
PFS is similar in patients with CCyR
regardless of the depth of molecular
response
18 months
1.0
0.9
0.8
Probability of PFS
CCyR with no MMR, n=91
0.7
CCyR with MMR, n= 41
0.6
p= 0.4
0.5
0.4
0.3
0.2
0.1
0.0
0
6
12
18
24
30
36
42
48
54
60
Months from starting imatinib therapy
Marin et al, Blood 2008
PFS similar in patients with CCyR regardless of
depth of molecular response
Druker BJ, et al. NEJM, 2006;355(25):2408-17.
PFS is similar in patients with CCyR regardless
of depth of molecular response
Kantarjian HM, et al. Blood. 2006;108:1835-1840.
Probability of loss of CCyR according
to the level of molecular response
1.0
CCyR with no MMR, n= 92
0.9
0.8
CCyR with MMR, n= 32
0.8
0.7
p= 0.04
0.6
0.5
0.4
0.3
23.9%
0.2
Probability of loss of CCyR
Probability of loss of CCyR
1.0
12 months
0.9
18 months
CCyR with no MMR, n=91
CCyR with MMR, n= 41
p= 0.006
0.7
0.6
0.5
0.4
24.6%
0.3
0.2
0.1
2.6%
0.0
0.1
0%
0.0
0
6
12
18
24
30
36
42
48
Months from starting imatinib therapy
54
60
0
6
12
18
24
30
36
42
48
54
60
Months from starting imatinib therapy
Marin et al, Blood 2008
The definition
of MMR is
wrong
Do not be
silly!
Problems with MMR
• The depth of the molecular response in a given patient is
basically driven by the patient’s adherence to therapy
• The definition of MMR is arbitrary
Problems with MMR
• The depth of the molecular response in a given patient is
basically driven by the patient’s adherence to therapy
• The definition of MMR is arbitrary
There is a great variability in the
response to imatinib. I wonder why
BCR-ABL/ABL ratio (%)
100
10
CCyR
1
3 log
0.1
0.01
0.001
0.0001
Time from start of imatinib
Study design
BCR/ABL/ABL ratio (%)
100
•
•
•
•
•
•
•
•
•
10
1
Imatinib
plasma
level
MEMS
0.1
0.01
0.001
TKD
mutations
Time from start of imatinib
hOCT1 level
MDR-1 polymorphisms
BCR-ABL transcript type
BCR-ABL transcript level
Sokal score
Hb
WBC
Sex
Age
We correlated all these variables with the
molecular response achieved by the patient
Microelectronic Monitoring System
(MEMS 6 Trackcap)
• Records the time of opening
the container
• Most reliable method of
measuring adherence
• Our patients: not told about
the chip
Long term adherence to imatinib
90
Proportion of patients (%)
80
70
60
50
40.2%
40
30
20
25.3%
13.8%
12.6%
10
8%
0
<80%
80–90% 90–95% 95–99% ≥100%
Percentage of intended dose
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
Lack of adherence
is underestimated by conventional methods
100
Proportion of patients (%)
90
80
70
60
Self reporting
Pill count
MEMS
50
40
30
20
10
0
<80% 80–90% 90–95% 95–99% ≥100%
Percentage of intended dose
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
Well, some
patients miss a
few doses,
so what?
Achievement of a molecular response is
related to the adherence to imatinib therapy
6-year probability of response
Adherence rate
100%
<99%
>95%
<95%
>90%
<90%
>85%
<85%
>80%
<80%
n
MMR (%)
4-log (%)
CMR (%)
36
51
p=0.01
91.1
58.6
p=0.02
79.9
38.6
p=0.02
46.7
22.7
57
30
p<0.001
94.5
29.3
p<0.001
77.2
15.0
p=0.002
45.2
8.2
64
23
p<0.001
93.7
13.9
p<0.001
76.0
4.3
p=0.002
43.8
0
69
18
p<0.001
85.8
11.8
p=0.001
69.2
5.6
p=0.007
40.8
0
75
12
p=0.001
81.2
0
p=0.005
63.8
0
p=0.04
37.1
0
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
6-year probability of MMR according to
the measured adherence rate
p<0.001
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
6-year probability of CMR according to
the measured adherence rate
p=0.002
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
Other variables are also predictive for the
achievement of molecular response
Variables
n
MMR (%)
4-log (%)
CMR (%)
40
47
p=0.036
59.2
80.7
1.186, p=0.012
p=0.03
39.5
69.1
1.323, p=0.01
p=0.011
14.7
47.6
1.209, p=0.07
Leukocytes
≤140 x 109/l
>140 x 109/l
RR
44
43
p=0.012
78.8
63.1
0.996, p=0.008
p=0.022
56.7
37.6
0.996, p=0.015
p=0.17
35.4
28.1
0.996, p=0.11
BCR-ABL1/ABL1 ratio
≤100%
>100%
RR
44
43
p=0.25
71.4
52.6
0.996, p=0.44
p=0.038
53.0
26.6
0.971, p=0.002
p=0.1
32.7
8.4
0.979, p=0.13
hOCT1 transcript level
≤0.16
>0.16
RR
30
30
p<0.001
55.2
81.4
2.199, p<0.001
p=0.01
42.0
64.8
1.990, p=0.001
p=0.02
16.6
45.3
1.665, p=0.04
43
41
p=0.02
60.1
83.2
2.11, p=0.01
p=0.07
53.0
68.0
2.50, p=0.06
p=0.14
23.3
44.4
2.25, p=0.09
64
23
p<0.001
93.7
13.9
1.093, p<0.001
p<0.001
76.0
4.3
1.104, p=0.002
p=0.002
43.8
0
RR= 1.135, p=0.012
Hemoglobin
≤115 g/l
>115 g/l
RR
Imatinib plasma level
≤1 g/ml
>1 g/ml
RR
Adherence rate
>90%
≤90%
RR
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
But adherence to therapy is the critical factor
for achieving molecular response
• MMR
– adherence to imatinib therapy, RR=11.17 (p=0.001)
– hOCT1 transcript level, RR=1.79 (p=0.038)
• CMR
– adherence to imatinib therapy, RR=19.35 (p=0.004)
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
Imatinib plasma levels are not an independent
predictor of molecular response
Total population
Marin D, et al. J Clin Oncol 2010; 28(14): 2381–2388.
Adherent patients
Who will sustain CCyR?
Study design
BCR/ABL/ABL ratio (%)
100
•
•
•
•
•
•
•
•
•
10
1
MEMS
0.1
0.01
0.001
Time from start of imatinib
hOCT1 level
MDR-1 polymorphisms
BCR-ABL transcript type
BCR-ABL transcript level
Sokal score
Hb
WBC
Sex
Age
We correlated all these variables with the
molecular response achieved by the patient
Poor adherent patients have a higher probability of
losing the CCyR and a lower EFS
1.0
1.0
0.9
0.9
0.8
0.8
Probability of imatinib failure
Cumulate incidence of loss of CCyR
p<0.0001
Adherence rate ≤85%, n=18
0.7
Adherence rate >85%, n=69
0.6
0.5
0.4
0.3
0.7
p<0.0001
0.6
0.5
0.4
0.3
0.2
0.2
Adherence rate ≤85%, n=18
0.1
0.1
Adherence rate >85%, n=69
0.0
0.0
0
6
12
Months from enrolment
18
24
0
6
12
Months from enrolment
18
24
Ibrahim, Blood 2011
On multivariate analysis, the adherence rate and
having failed to achieve a major molecular
response are the only independent predictors for
loss of CCyR and discontinuation of imatinib
therapy.
Ibrahim, Blood 2011
Adherence and the achievement of MMR are the
only independent predictors for outcome
1.0
1.0
p<0.0001
0.9
MMR, n=53
0.8
Probability of imatinib failure
Cumulate incidence of loss of CCyR
0.9
CCyR, no MMR, Adherence Rate ≤85%, n=11
0.7
CCyR, no MMR, Adherence Rate >85%, n=23
0.6
0.5
0.4
0.3
p<0.0001
0.2
p=0.0009
p=0.003
0.8
0.7
0.4
0.3
0.0
0.0
12
Months from enrolment
18
24
MMR, n=53
0.2
0.1
6
p<0.0001
0.5
0.1
0
p<0.0001
0.6
CCyR, no MMR, Adherence Rate ≤85%, n=11
CCyR, no MMR, Adherence Rate >85%, n=23
0
6
12
18
Months from enrolment
24
Ibrahim, Blood 2011
Problems with MMR
• The depth of the molecular response in a given
patient is basically driven by the patient’s
adherence to therapy
• The definition of MMR is arbitrary
1013
Metaphases
100
Ph +
Ph Ph +
Ph +
10
MCyR
1011
Ph -
Ph -
1
CCyR
1010
CCyR
Metaphases
109
0.1
MMR
Ph -
0.01
108
0.001
107
Total number of leukaemia cells
MiCyR
BCR/ABL/ABL ratio (%)
1012
CHR
166 out of 282 patients who received imatinib as
first line therapy were in CCyR at 12 months
Transcript
level
>0.1%
<0.1%
125
41
OS
(%)
EFS
(%)
p=0.5
94.2
96.3
p=0.08
80.4
93.7
166 out of 282 patients who received imatinib as
first line therapy were in CCyR at 12 months
Transcript
level
>0.1%
<0.1%
>0.53
<0.53
OS
(%)
EFS
(%)
125
41
p=0.5
94.2
96.3
p=0.08
80.4
93.7
20
146
p=0.01
81.5
94.4
p<0.0001
29.5
74.3
It can not be a
talk about CML
without
mentioning KD
mutations
I am going to try to challenge the orthodox
view about kinase domain mutations
The points I want to make are:
• The meaning of KD mutations is often
misunderstood
• The uses in clinical practice are very
limited
Sensitivity studies
help us to choose
the best antibiotic.
Similarly mutation
analysis help us to
choose the best TKI
Are you sure?
Dasatinib 100 mg QD in CML-CP: 24-month data (034)
Figure 3. MCyR rates in patients with or without
a baseline BCR-ABL mutation
80
60
Any BCR-ABL mutation
55
%
14
54
56
No BCR-ABL mutation
70
67
66
67
12
22
0
ASH 2008
10
58
58
57
11
54
41
11
48
8
40
20
8
46
34
37
100 mg 70 mg 140 mg 50 mg
once
BID
once
BID
daily
daily
(n=49) (n=50) (n=50) (n=63)
100 mg 70 mg 140 mg 50 mg
once
BID
once
BID
daily
daily
(n=98) (n=96) (n=89) (n=86)
PCyR
CCyR
100
100
10
75
1
50
0.1
25
0.01
0
Imatinib:
400
800
600
1000
Percentage of mutant transcripts
BCR/ABL/ABL ratio (%)
Group A, High transcript levels- mutant clone predominates
0.001
0.0001
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
M244V
Time since the onset of imatinib therapy (months)
Interval from diagnosis to start of imatinib: 4 months
Khorashad, Leukemia 2006
100
100
10
75
1
50
0.1
25
0.01
0
Imatinib: 400
600
400
Percentage of mutant transcripts
BCR/ABL/ABL ratio (%)
Group B, Low transcript levels- mutant clone predominates
0.001
S438C
0.0001
0
3
6
9
12 15 18 21 24 27 30 33 35 36 39 42 45
Time since the onset of imatinib therapy (months)
Interval from diagnosis to start of imatinib: 2 months
Khorashad, Leukemia 2006
100
100
10
75
1
50
0.1
25
0.01
0
Percentage of mutant transcripts
BCR/ABL/ABL ratio (%)
Group C, Variable transcript levels- mutant clone is rare
Imatinib: 400
0.001
0.0001
0
3
6
9
12 15 18 21 24 27 30 33 35 36 39 42 45
G250E
Time since the onset of imatinib therapy (months)
Interval from diagnosis to start of imatinib: 36 months
Khorashad, Leukemia 2006
What is the biological significance
of KD mutations?
In order to answer this question we
systematically screened all our CP (n=319)
patients treated with imatinib for mutations
regardless of whether or not they shown
any sign of resistance
Mutation screening
Mutation=0
Mutation=M244V, 55%
undetectable 5%
12 m
20%
18 m
Khorashad et al, JCO, 2008
Cumulative Incidence of KD Mutations
Cumulative incidence of KD mutations
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
13.9%
0.1
0.0
0
6
12
18
24
30
36
42
48
54
60
Months from starting imatinib therapy
Khorashad et al, JCO, 2008
Mutations in Patients who Achieved CCyR
214 CCyR patients: 6 (3%) with mutations
All of them lost CCyR
T315I, L387M, S417F, E459K, G459K, and M351T
Median interval from mutation detection to loss of
CCyR: 20.8 months
Median interval from mutation detection to any
change in the BCR-ABL transcript level: 12 months
Khorashad et al, JCO, 2008
The Development of Mutation Predicts for the Loss
of CCyR
KD mutation was the only predictive factor for loss of
CCyR in the multivariate analysis:
RR=3.8, p=0.005
Khorashad et al, JCO, 2008
Example 1
Panel A, patient 34 (E459K)
BCR/ABL/ABL ratio (%, blue)
100%
Doubling
transcript levels
CCyR
75%
10
BP
1
50%
25%
0.1
Loss of CCyR
0.01
0.001
First detection of
mutation
0.0001
0
1
2
3
4
5
6
7
8
9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Time since the onset of imatinib therapy (months)
0%
Percentage of mutant transcripts (%, red)
100
Example 2
Panel B, patient 29 (M351T)
BCR/ABL/ABL ratio (%, blue)
CCyR
Loss of CCyR
Doubling
transcript levels
75%
10
v
1
50%
v
0.1
25%
0.01
0%
First detection of
mutation
0.001
0.0001
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
Time since the onset of imatinib therapy (months)
48
51
54
57
60
63
Percentage of mutant transcripts (%, red)
100%
100
Prognostic Impact on PFS
Among 319 patients, 49 (15%) progressed to advanced
phase
17 of 49 (35%) had a mutation detected before progression
14 of 17 had a mutation detected while still in CHR
median interval (detection-progression): 16.3 months
median interval (detection-loss of CHR): 13.7 months
Khorashad et al, JCO, 2008
Prognostic Impact on PFS
Multivariate analysis in the whole population (m=319),
showed that KD mutations and the achievement of CCyR
are the only independent predictor for PFS
CCyR (RR=0.15, p<0.0001)
Mutation detection (RR=2.3, p=0.014)
Khorashad et al, JCO, 2008
Landmark at 2 Years, PFS
CCyR vs no CCyR
Mutation vs. no mutation
90%
1.0
0.9
0.8
66%
0.7
0.6
-- CCyR (n=143)
-- no CCyR (n=107)
0.5
0.4
0.3
0.2
P< 0.0001
0.1
0.0
0
6 12 18 24 30 36 42 48 52 60 66 72 78 84
Months from starting imatinib therapy
0.8
Probability of PFS
Probability of PFS
84%
1.0
0.9
0.7
0.6
35%
0.5
0.4
--’no mutation’ group (n=225)
--’mutation’ group (n=25)
0.3
0.2
P= 0.0001
0.1
0.0
0
6 12 18 24 30 36 42 48 52 60 66 72 78 84
Months from starting imatinib therapy
Khorashad et al, JCO, 2008
Conclusion
TKD mutations are mere surrogate markers for
genetic instability and in many cases are not the
real reason for resistance
Khorashad et al, JCO, 2008
How should we use the mutation
screening in practice?
A. Perform a mutation analysis on a regular
basis (i.e every 3 months) regardless of
any sign of resistance
– Caveat: it is extremely cost ineffective
B. Perform mutation analysis only at the
moment of switching therapy
EHA 2009
BCR-ABL mutation status before starting dasatinib.
Frequency of baseline BCR-ABL mutations
by in vitro IC50 to dasatinib (N=1043)
Unknown IC50 to dasatinib (n=83)
43 different BCR-ABL mutations
8%
No BCR-ABL
mutation
(n=641)
24%
61%
IC50 ≤3 nM (n=254)
M244V, G250E,
Y253F/H/K, F311L,
M351T, E355G,
F359C/I/V, V379I,
L387M, H396P/R
<1% V299L (n=1)
1% Q252H (n=6)
1% F317L (n=14)
2% E255K/V (n=25)
2% T315I (n=21)
IC50 >200 nM
IC50 >3 nM
(n=44)
4%
Müller M, et al. ASH 2008: Abstract 449.
2G-TKD mutations
• Dasatinib: T315I, T315A, V299L F317V, F317L
• Nilotinib: T315I, Y253F, Y253H, E255V, E255K
You agree with me if
you think that:
1. What matters is whether the patient is resistant,
not if a mutation is present.
2. Mutation analysis may be helpful in choosing a
2G-TKI in 5%-10% of the cases
3. Mutations are surrogate marker for genomic
instability
Thanks to John Goldman
and other friends who are too numerous to be
mentioned individually
David, Thankfully
your patients fare
better than your
plants