amphotericin B
advertisement

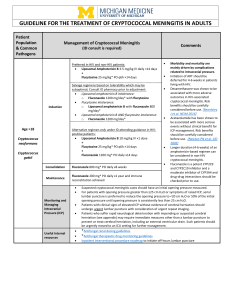
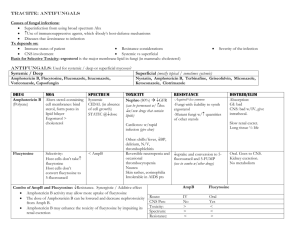
Department of Pharmacology College of Medicine Our Lady of Fatima University CASE NO. 24 By: Ramos Jr., Nicandro and Joseph Yang INTRODUCTION A patient with CLL presented with headache, visual disturbances and stiff neck. He was admitted to a hospital and spinal tap was performed. Cryptococcus neoformans was isolated from the spinal fluid and the patient was begun on amphotericin-B. The expected toxicity of this drug occurred, and in fact, he was switched to 5-fluorocytosine. INTRODUCTION DIAGNOSIS - Chronic Lymphocytic Leukemia (CLL) PATIENT SYMPTOMS - headache - visual disturbances - stiff neck INTRODUCTION LABORATORY TEST SPINAL TAP (+) Cryptococcus neoformans INTRODUCTION Prior medication • Amphotericin- B Current medication • 5- Fluorocytosine CASE: GUIDE QUESTIONS 1. Potential toxicities related to Amphotericin-B theraphy. 2. Is the therapy describe optimal? 3. Anephric patient – which AF drug might be choose? 4. If this patient had AIDS with Cryptococcal meningitis, what would constitute the usual induction & maintenance therapy? DEFINITIONS • CLL - acquired injury to the DNA of a single cell, a lymphocyte in the bone marrow that results in “uncontrolled growth” of CLL cells – Increase Blood level of Lymphocytes DEFINITIONS • Cryptococcus neoformans -a fungus -very common in the soil -can get into your body when you “breathe in” dust or dried bird droppings -can travel through the blood to the spinal column and brain Nicky’s CLINICAL IMPRESSION Cryptococcal Meningitis specific: Cryptococcus neoformans Related to: - CLL - patient is immunocompromised Nicky’s CLINICAL IMPRESSION Cryptococcal Meningitis • Moderate-to-Severe -CSF sample (+)Cryptococcus neoformans. - Brain-related symptoms of disease (e.g. severe headaches, vision disturbance) AMPHOTERICIN-B • • • • • Systemic AF Produced- Streptomyces nodolus Amphoteric polyene macrolide Nearly insoluble in H2O deoxycholate (Fungizone™) -colloidal suspension of amphotericin B • bile salt, deoxycholate -used as the solubilizing agent. AMPHOTERICIN-B PREPARATIONS Amphotericin B Colloidal Dispersion (ABCD; Amphocil™ or Amphotec™) Amphotericin B Lipid Complex (ABLC; Abelcet™) Liposomal Amphotericin B (L-AMB; Ambisome™) CHEMICAL STRUCTURE AMPHOTERICIN-B PHARMACOKINETICS • GIT – poor absorption • Oral form-not used for systemic infections • Serum T1/2 – 15 days • Intrathecal therapy – Fungal meningitis AMPHOTERICIN-B MECHANISM OF ACTION • binds to cell membrane sterol, ergosterol • binding disrupts osmotic integrity • result in leakage of intracellular potassium, magnesium, sugars, and metabolites • cellular death AMPHOTERICIN-B MECHANISM OF ACTION AMPHOTERICIN-B ANTIFUNGAL ACTIVITY • Broad spectrum • Candida albicans • C. neoformans • H. capsulatum • B. dermatitis • C. immitis • P. boydii • Aspergilus fumigatus and mucor AMPHOTERICIN-B ADVERSE EFFECTS • Fever, chills, muscle spasm • Vomiting, headache • Hypotension • abnormal liver function • Seizures • Chemical arachnoiditis • NEPHROTOXICITY “did happen to our patient” AMPHOTERICIN-B ADVERSE EFFECTS • • • • Nephrotoxicity generally reversible, up to 10% Irreversible > 4g cumulative dosing ”possible dose for our patient” dose and duration dependent two mechanisms: – 1) the effects on renal blood flow and glomerular filtration – 2) the direct toxic effects on (primarily) the distal tubules. AMPHOTERICIN-B ADVERSE EFFECTS Nephrotoxicity 5 - FLUOROCYTOSINE • • • • • • • • Antimetabolites (only) - AF 1950's -potential antineoplastic agent A.k.a. -flucytosine (5-FC) 4-amino-5-fluoro-2-pyrimidone Water soluble Pyrimidine analog activated by deamination marketed - AncobonTM 5 - FLUOROCYTOSINE PHARMACOKINETICS • • • • Oral formulation only 37.5 mg/kg/day 4X/day Poorly protein bound Well penetration in all BF compartments (CSF) • Renal toxicity 5 - FLUOROCYTOSINE MECHANISM OF ACTION • inhibits protein synthesis by replacing uracil with 5-flurouracil in RNA. • inhibits thymidylate synthetase via 5fluorodeoxy-uridine monophosphate and thus interferes with fungal DNA synthesis 5 FLUOROCYTOSINE MECHANISM OF ACTION 5 - FLUOROCYTOSINE ANTI FUNGAL ACTIVITY • Candida spp. • Cryptococcus neformans • Aspergillus spp. • dematiaceous fungi • Phialophora spp. • Cladosporium spp. – causing chromoblastomycosis 5 - FLUOROCYTOSINE ADVERSE EFFECTS • Gastrointestinal intolerance • bone marrow depression (anemia, leukopenia, thrombocytopenia) • Rash • hepatotoxicity • Headache • Confusion, hallucinations, sedation, euphoria CASE: GUIDE QUESTIONS 1. Potential toxicities related to Amphotericin-B theraphy. “NEPHROTOXICITY” (primary) • Fever, chills, muscle spasm • Vomiting, headache • Hypotension • abnormal liver function CASE: GUIDE QUESTIONS 2. Is the therapy describe optimal? Ideally : •First two weeks of treatment, the drug amphotericin B (Fungizone®) is given every day through an IV line • Along with a second drug taken: •orally flucytosine (Ancobon®). CASE: GUIDE QUESTIONS IDEAL THERAPY 1-2 weeks 5-FC amphotericin-B Lab Test CSF or Blood Continue 5-FC amphotericin-B Lab Test CSF or Blood (+) C.neo (-) C.neo Discontinue fluconazole (Diflucan®) oral 200mg to prevent recurrence STOP (6mo) Good Immune system (-) C. neo Next reporter 3. If the patient were anephric, which antifungal agent might one choose? • The choice of antifungal agents could be a combination of Amphotericin B and Flucytosine(5-FC) for systemic fungal infection, such as cryptococcal meningitis. But this therapy is useful only when the patient had a normal renal function with hemodialysis, since both drugs have very strong nephrotoxicity. • The irreversible form of amphotericin nephrotoxicity usually occurs in the setting of prolonged administration. • The Flucytosine (5–FC) nephrotoxicity is more likely to occur in the presence of renal insufficiency and in AIDS patients. • So, in renal insufficient patients, the systemic anti-fungal agent of choice is Azoles, which are relatively nontoxic and have mostly hepatic elimination route. The most common adverse reaction is relatively minor gastrointestinal upset and abnormalities in liver enzymes. Ketocon- Itraconazole azole Fluconazole Voriconazole Water low solubility low high high Absorption variable variable high high Half life 7-10 24-42 23-31 6 CSF:Se- <0.1 rum ratio <0.01 >0.7 …. ketokona zole Itraconazo Fluconaz Voriconaz le ole le Elimination hepatic hepatic renal hepatic Formulations oral Oral,IV Oral,IV Oral,IV Azol of Choice No more systemic use in USA due to high inhibition of P450 Indermato phytoses, onychomy cosis and Aspergillus sp. Cryptoco ccal meningitis Good against Candida species, including C. Krusei and FLUCONAZOLE • Excelent CSF penetration • DOC – C. neoformans FLUCONAZOLE Mechanism of Action • inhibit cytochrome P-450 3-A dependent enzyme 14-alpha demethylase • interrupting the synthesis of ergosterol. • depletion of ergosterol in the cell membrane and accumulation of toxic intermediate sterols, • causing increased membrane permeability and inhibition of fungal growth. FLUCONAZOLE Mechanism of Action • Besides Azoles, Liposomal Amphtericin B has been developed for less nephrotoxicity, • It is specially formulated as lipid- vehicled drug is less likely to bind to the human cholesterol and more likely to bind into fungal ergosterol in fungal cell membrane. 4. If this patient had AIDS with cryptococcal meningitis, what would constitute the usual induction therapy and maintenance therapy? • The answer is Fluconazole. The drug of choice is following reasons. I. Prophylactic use of Fluconazole has been demonstrated to reduce fungal diseases in bone marrow transplant recipients and AIDS patients. II. Fluconazole is the azole of choice in the treatment and secondary prophylaxis of cryptococcal meningitis because 1. It displays a good cerebrospinal fluid penetration. 2. Unlike other Azoles (ketoconazole and itraconazole), its oral bioavailavility is high. 3. Drug interactions are also less common because Fluconazole has the least effect of all the azoles on hepatic microsomal enzymes. Thank You!! Any questions? CASE: GUIDE QUESTIONS 4. If this patient had AIDS with Cryptococcal meningitis, what would constitute the usual induction & maintenance therapy? Diagnosed early: • two weeks of amphotericin B followed by oral fluconazole. • fluconazole is continued for life. Without it, the meningitis is likely to come back. CASE: GUIDE QUESTIONS Compromised immune systems (less than 50 T-cells), • fluconazole (Diflucan®), an oral pill (200 mg) taken once a day, to help prevent cryptococcal meningitis DRUGS USED FOR CLL alemtuzumab (Campath®) chlorambucil (Leukeran®) cladribine (Leustatin®) cyclophosphamide (CYTOXAN®) doxorubicin (Adriamycin®) fludarabine (Fludara®) prednisone (Deltasone®) vincristine (Oncovin®) 5 - FLUOROCYTOSINE DRUG INTERACTIONS • flucytosine + amphotericin B • renal impairment caused by amphotericin B may increase the flucytosine levels • thus potentiate its toxicity • toxicity of flucytosine is presumably due to 5fluorouracil - produced from flucytosine by intestinal bacteria