PowerPoint bemutató
advertisement

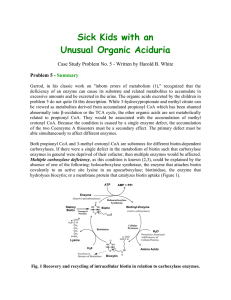
Biotinidase deficiency: clinical presentation, treatment and screening Ferenc Papp University of Szeged, Department of Pediatrics Biotinidase deficiency Inherited disorder of biotin metabolism The body cannot recycle endogenous biotin and develop a secondary biotin deficiency Biotin Water-soluble essential B-complex vitamin (vitamin H) Cofactor for all 4 carboxylase enzymes: pyruvate caboxylase (gluconeogenesis) acetyl-CoA carboxylase (fatty acid synthesis) propionyl-CoA carboxylase (Ile, Val, Met, Thr catabolism) methylcrotonyl-CoA carboxylase (Leu catabolism) Dietary biotin is bound to proteins Free biotin is generated in the intestine by digestive enzymes, by bacteria and by biotinidase Dietary biotin protein-bound Proteolytic enzymes Bacteria Biotinidase MULTIPLE CARBOXYLASE DEFICIENCY JUVENILE/LATE FORM Lysine MULTIPLE CARBOXYLASE DEFICIENCY INFANTILE/EARLY FORM Free biotin Holocarboxylase synthase Biotinidase Biocytin Apocarboxylases Biotin cycle Proteolytic degradation Apocarboxylases Pyruvate Acetyl-CoA Propionyl-CoA Methylcrotonyl-CoA Biotin Holocarboxylases Protein catabolism Fatty acid synthesis Gluconeogenesis Biotinidase deficiency Two types: Profound < 10% of mean normal enzymatic activity Partial 10-30% reduced activity Epidemiology Incidence of profound and partial deficiency is 1:60.000 in most countries Brazil 1:9.000 Relatively common in Hungary estimated combined incidence is 1:23.000 58 children had decreased biotinidase activity from 1.336.145 newborns (1989-2001, László et al., 2002) clinical, biochemical and genetic characterization of 20 pts (11 profound, 7 partial, 2 heterozygous) Genetic background Autosomal recessive inheritance BTD gene 3p25, 4 exons > 140 disease-causing mutations Spectrum and frequency of mutations are considerably variable in different ethnic groups 5 mutations are very common in Caucasians: p.D444H, p.Q456H, p.R538C, p.A171T:D444H, c.98:d7i3 Genetic background p.D444H mutation causes 50% reduction in enzyme activity and is almost always associated with partial deficiency In partial form p.D444H is combined with a severe mutation 10 to 30% enzyme activity Patients with complete deficiency have two severe mutations less than 10% enzyme activity Clinical presentation There is considerable variability of clinical features as well as age of onset of symptoms in enzyme-deficient children Symptoms may appear from several months to several years of age but may develop as early as 1 week of age (term late form does not apply to all cases!) First clinical symptoms appear between 3-6 months of age in most of the cases Symptoms can be seen mostly, but not only in profound form and in pts without treatment Clinical presentaion Skin manifestations Neurological symptoms Hearing loss, eye problems Immunodeficiency (fungal and bacterial infections) Gastrointestinal problems (nausea, vomiting, anorexia) Metabolic decompensation with acidosis and organic aciduria Cutaneous findings Dry skin Seborrheic dermatitis Ekzema Rashes Fine and brittle hair Hair loss or total alopecia Fungal skin infections Neurological symptoms Hypotonia Ataxia Lethargy Myoclonic seizures Developmental delay Mental retardation Hearing loss Visual problems Clinical data of 37 symptomatic pts with profound biotinidase deficiency were analysed (Pomponio et al., USA, Ped Res, 1997) Age of onset: 1 to 180 months (mean 11.8) Symptoms improved or resolved after therapy and the children have remained asymptomatic while taking biotin In some pts the residual neurologic damage has continued Symptoms No. of pts % (total 37) Rash 25 67 Hypotonia 25 67 Seizures 23 62 Hearing deficits 23 62 Lethargy 22 59 Alopecia 22 59 Ataxia 18 48 Visual problems 14 38 Mental retardation 11 30 Gastrointestinal 8 21 Fungal skin infection 5 13 Laboratory findings Metabolic acidosis, ketosis, hyperammonaemia Elevated C3 and C5OH detected by MS/MS Pathological organic acid profile in the urine (propionic acid, methylcitrate, 3-methylcrotonic-, 3hydroxyisovaleric acid, 3-methylcrotonylglycine) These lab findings can be observed mostly in untreated pts or in metabolic decompensation Diagnosis Based on detection of decreased biotinidase activity in the blood and/or in the serum compared to a normal control by using colorimetric test DNA testing is also available, but this is not necessary for confirmation of biotinidase deficiency Treatment Pharmacologic dose of biotin resolves many of the clinical features in symptomatic pts and prevents the development of symptoms in asymptomatic pts Recommended daily dose is 5-20 mg orally Lifelong treatment is needed (carriers do not need therapy) Hearing loss, eye problems and developmental delay do not resolve completely with biotin therapy Early diagnosis and treatment are needed before permanent neurologic damage occurs Screening A colorimetric method for diagnosing of biotinidase deficiency was developed by Knappe (1963) It was adopted for newborn screening by Heard (1984) In Hungary screening was introduced in 1989 Biotinidase deficiency has been screened in 47 of 51 states of the USA and in 6 European countries (Sweden, Germany, Switzerland, Austria, Lichtenstein and Hungary) at 2007 Screening has been started in 4 more European countries with pilot studies at the same time (Spain, Belgium, Italy, Turkey) Screening method A quantitative colorimetric method is used Enzyme activity is measured directly in the DBS Result is not influenced by days of life, gestational age or breast feeding Only transfusion of a newborn can interfere with biotinidase screening, in that case screening needs to be repeated at the age of 2 weeks and 60 days Summary Inherited disorder of biotin recycling Two severity forms: profound and partial If left untreated affected individuals develop severe clinical abnormalities In symptomatic pts mostly neurologic and cutaneous complications can be observed It can be treated effectively with biotin supplementation Summary Permanent neurologic symptoms do not resolve with therapy Early diagnosis is very important, so that therapy can be initiated before clinical symptoms appear Clinical consequencies of biotinidase deficiency can be minimized effectively by newborn screening