Overview")
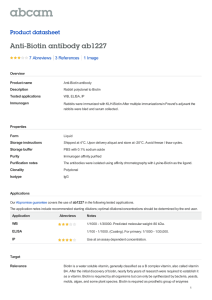
Biotinidase Deficiency (BTD) INTRODUCTION Our body requires biotin, a water-soluble B-vitamin that is required for metabolism in the body. 4 It acts as a cofactor for carboxylation reactions needed for gluconeogenesis, lipid 4 metabolism and amino acid catabolism. There are a variety of carboxylases that require biotin 4 in order to facilitate carboxylation reactions. It is vital that the necessary enzymes are present to complete their role in these metabolic pathways. CLASSIFICATION OF SYMPTOMS Based on residual enzyme activity PROFOUND DEFICIENCY (10% of normal enzymatic activity) Seizures Hypotonia Delayed development Cutaneous manifestations Optic atrophy Hyperventilation Hearing loss WHAT IS BIOTINIDASE DEFICIENCY Biotinidase is an important enzyme required for the formation of biotin through a series of 1 reactions known as biotin turnover and biotin recycling. Without this enzyme, there is a reduction of free biotin available to act as cofactors leading to multiple carboxylase 2 deficiency, where the carboxylases are unable to function. Biotinidase also plays a vital role in the central nervous system (CNS) where it is localized to red nucleus and cerebellar 2 purkinje cells. This makes the enzyme an important aspect to proper CNS function. PARTIAL DEFICIENCY (10-30% of normal activity) Biotinidase deficiency is an autosomal recessive disease that results in reduced or absent biotinidase activity. 2 The cause of the disease are mutations in the BTD gene which prevents the recycling of biotin within the body leading to a series of symptoms. Symptoms only during metabolic stress: - skin rash - hair loss BIOCHEMICAL PROCESSES BIOTIN 2,7 SOURCES: Figure 2. Image representation of biotinidase symptom of hair loss cooked egg Organ meats Fish Sweet potatoes Broccoli Incidence 3 1 in 60, 000 KEY POINTS Figure 3. artistic representation of skin rash Figure 1. Describes the biotin cycle where free biotin obtained from the diet binds to various apocarboxylases (inactivated carboxylases), done by holocarboxylase synthetase. The listed apocarboxylases involved are: propionyl-CoA carboxylase (PCC), beta-methylcrotonyl-CoA carboxylase (MCC), pyruvate carboxylase (PC) & acetyl-CoA carboxylase (ACC). The action done by the holocarboxylase synthetase results in a holocarboxylase which is broken down to form biocytin and cleaved by biotinidase to remove a lysine, ultimately recycling the biotin. Adapted from: Fig. 1., Devanapalli et al. 1 Our body received biotin from the diet and microbiota, and in doing so, this acts as a source of free biotin. The free biotin is then attached onto apocarboxylases and this results in holocarboxylases. These holocarboxylase are necessary for carboxylation reactions in important metabolism pathways including amino acid metabolism, fatty acid synthesis and gluconeogenesis. These enzymes are then broken down into biocytin which is then able to be turned into biotin when lysine is removed. To treat this condition, there is a requirement for an increase in free biotin levels due to the individual’s inability to recycle the biotin. Without the recycling ability of biotin means that there is a requirement for biotin levels to be adjusted through receiving it from the environment. This can be supplemented either through consumption of foods with biotin, or 7 biotin supplements. DIAGNOSIS 6 Abnormal Newborn screening: This can be detected through the use of fluorescent or colorimetric tests to determine biotinidase activity Symptomatic individual: Atypical findings associated with partial biotinidase deficiency Lab findings: Metabolic ketaactic acidosis TREATMENT 5,7 5-10 mg/day for those who have <10% mean normal serum enzyme activity 2.5-10 mg/day for those who have Daily administration of oral biotin (initiated early) Prevent clinical symptoms given presymptomatic diagnosis & early treatment Biotinidase is a vital part of our ability to recycle biotin in our body, which plays an integral role in many metabolism pathways of our body. With a deficiency, this leads to the inability to properly metabolize lipids, amino acids and hinder the process of gluconeogenesis. Early detection is key in managing the development of symptoms and prevention of severe symptoms. Support from family and community is important as an individual navigates their life with this disease. Educational resources are also available for further information. REFERENCES 1. Arslan M, Oksuz Y, Kizilboga B, et al. A patient diagnosed with Li-Campeau syndrome and biotinidase deficiency. J Pediatr Acad. 2023;4(3):113+. doi:10.4274/jpea.2023.221. 2. Devanapalli B, Wong RSH, Lim N, et al. Biotinidase deficiency: A treatable neurometabolic disorder. Brain Dev Case Rep. 2024;2(2):100021. doi:10.1016/j.bdcasr.2024.100021 3. Kannan B, Navamani HK, Jayaseelan VP, Arumugam P. A Rare Biotinidase Deficiency in the Pediatrics Population: GenotypePhenotype Analysis. J Pediatr Genet. 2022;12(1):1-15. Published 2022 Nov 1. doi:10.1055/s-0042-1757887 4. Perry CA, Butterick TA. Biotin. Adv Nutr. 2024;15(7):100251. doi:10.1016/j.advnut.2024.100251 5. Radelfahr F, Riedhammer KM, Keidel LF, et al. Biotinidase deficiency: A treatable cause of hereditary spastic paraparesis. Neurol Genet. 2020;6(6):e525. Published 2020 Oct 13. doi:10.1212/NXG.0000000000000525 6. Tankeu, A. T., Van Winckel, G., Elmers, J., Jaccard, E., Superti-Furga, A., Wolf, B., & Tran, C. (2023, April). Biotinidase deficiency: What have we learned in forty years?. Molecular Genetics and Metabolism. https://www.sciencedirect.com/science/article/pii/S1096719223001907 7. Wolf, B. (2000, March 24). Biotinidase deficiency. In M. P. Adam, J. Feldman, G. M. Mirzaa, et al. (Eds.), GeneReviews® [Internet]. University of Washington. Updated May 25, 2023. Available from https://www.ncbi.nlm.nih.gov/books/NBK1322/