Pertussis and Pertussis Vaccination: Why All the
advertisement

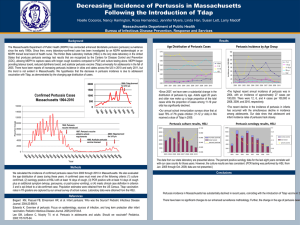
Disclosure Slide We have no financial relationships with any commercial interest related to the content of this activity Pertussis and Pertussis Vaccination: Why All the Whoop-la? A Summary for South Carolina Medical Providers Riyadh D. Muhammad, MD, MPH – Pediatrician Helen L. Huber, MSN - Pediatric Nurse Practitioner Bureau of Disease Control South Carolina Department of Health and Environmental Control Source: W. Orenstein. An overview of Vaccinology; 2009 Clinical Vaccinology Course, Atlanta. Sounds of Pertussis Whooping Child Whooping Adult Overview • Pertussis Surveillance Data • Clinical Considerations – – – – – Background Clinical Features Diagnosis Treatment Reporting cases to DHEC • Vaccine – – – – Vaccines available Recommendations Coverage rates Safety Reported Pertussis Cases* U.S., 1922-2009† DTP (1949) DTaP for doses 4 & 5 (1992) DTaP for all doses (1997) Tdap (2005) *National Notifiable Diseases Surveillance System (NNDSS) †2009 data provisional Ref: S. Roush, NIC 2010 Reported Pertussis Cases* Tdap U.S., 1980-2009† (2005) 1997: PCR included in case definition *National Notifiable Diseases Surveillance System (NNDSS) †2009 data provisional Ref: S. Roush, NIC 2010 U.S. Pertussis Cases, 2010 Ref: CDC. Unpublished data. Rate South Carolina S.C. Pertussis Cases, 2010 South Carolina, 2010 South Carolina Pertussis • Fastidious gram-negative bacillus, Bordetella pertussis • Severe, debilitating cough illness lasting weeks to months (“100 day cough”) • Characterized by paroxysms of cough, inspiratory whoop, vomiting; apnea in young infants Pertussis • Highly contagious • Transmission by contact with secretions, droplets from nose or mouth • Vaccine preventable, but poorly controlled – Despite high childhood vaccine coverage, pertussis remains a problem in S.C. and the U.S. Pertussis • Worldwide occurrence • Affects all ages, even vaccinated persons • Morbidity and mortality complications most common among infants – Transmission from parents, household members – Recommendation for cocooning vaccination approach • Persistent cough itself can cause complications Pertussis Clinical Features • Incubation period 5-10 days (range 4-21 days) • Insidious onset, similar to minor URI with nonspecific cough • Fever minimal or absent • Pertussis presentation varies depending upon age, existing immunity • Classically characterized by – Paroxysms of cough – Inspiratory whoop – Vomiting Timeline of Pertussis Symptoms • Catarrhal stage 1-2 weeks – Mild URI, progresses to cough – Most contagious stage • Paroxysmal cough stage 1-6 weeks – Whooping, vomiting • Convalescence – Gradual resolution Weeks to months Pertussis Epidemiology • Reservoir Humans • Transmission Respiratory droplets • Communicability Maximum in catarrhal stage Secondary attack rate up to 80% Pertussis Among Adolescents and Adults • Disease often milder compared to infants and children – Persons with mild disease may transmit the infection • Infection may be asymptomatic, or present as classic pertussis – Pertussis is unrecognized, underreported – Asymptomatic infections are 4 to 22 times more common than symptomatic infections – Symptomatic adolescents and adults are the major source of infection in unvaccinated children Pertussis Among Infants • Most severe disease • Infants under 6 months have an atypical presentation – Short catarrhal stage – Longer period of convalescence – Absence of whoop • Prominent symptoms can be – Gagging – Gasping – Apnea • Can lead to sudden unexplained death Let’s Protect Our Infants! Pertussis Deaths in the U.S., 2004-2006 Age at onset <3 mos >3 mos Total 2004 24 3 27 2005 32 7 39 2006 13 3 16 Total 69 13 82 (84%) (16%) CDC, unpublished data, 2007 Source of Pertussis Among Infants • 616 cases of pertussis in infants • Source identified in 264 (43%) – Parents 47% – Siblings 20% – Grandparents 8% – Other 25% Ref: Bisgard et al. PIDJ 2004;23:985-989. Pertussis Complications Condition Pneumonia Seizures Encephalopathy Hospitalization Death Percent reported 4.9 0.7 0.1 16 0.2 *Cases reported to CDC 2001-2003 (N=28,998) Pertussis Complications • Seizures • Encephalopathy • Syncope • Rib Fractures • Incontinence Courtesy of T. Schlenker, Children's Hospital of Wisconsin Pertussis Diagnosis • Culture • Polymerase chain reaction (PCR) • Serology • Direct fluorescent antibody (DFA) • DFA and serology might be clinically useful – Cannot be used for case confirmation for reporting Pertussis Diagnosis Is currently complicated by: – Stage of disease (catarrhal, paroxysmal, convalescent) – Antimicrobial administration – Vaccination status – Quality/timely collection of clinical specimen – Transport conditions – Contamination of clinical specimen – Lack of clinically validated and standardized tests 26 Optimal Timing for Pertussis Diagnostic Testing Communicable Period Incubation Period Catarrhal Stage -3 Symptom Onset 0 2 Convalescent Paroxysmal Stage Stage 8 Weeks Bacterial Culture PCR Serology 12 PCR Pros •High sensitivity •Results can be obtained quickly •Organism does not need to be viable •Less affected by immunization and antibiotics Cons •Expensive •No commercial FDA approved tests or standardized protocol •No standardized reagents or interpretation of results •Most labs only use single targets •False positives and contamination •Still affected by disease phase and antibiotic treatment Culture Pros Cons •Gold standard •100% specific •False positives not a concern •Low cost •Facilitates public health surveillance •Difficult collection, transport, growth conditions •Slow, incubation time up to 10 days •Lower yield if prior antibiotics •Low sensitivity -Generally 30-60%, but can be <10% for adolescents and adults with prolonged cough Isolation drastically declines after: - 2 weeks of cough - Antimicrobial or vaccine administration - Inappropriate collection/transport /growth conditions ‘Pseudo’ Outbreaks of Pertussis: Pitfalls of PCR Problems Identified in Pseudo Pertussis Outbreaks • Over reliance on PCR – Single, non-specific DNA targets – Few cultures were performed • Testing ill persons without typical pertussis symptoms – Viruses, parapertussis, Chlamydia, Mycoplasma, etc • Contamination of PCR tests via – Specimens from true cases – Pertussis vaccines • Inappropriate specimen handling Obtain PCR and Culture • CDC and DHEC recommend culture along with your PCR – PCR should be used in conjunction with and not in place of culture • Pertussis culture is – Cheap – Facilitates validation of PCR results – Keeps PCR ‘honest’ • False positives • Contamination • None are FDA approved Collecting Pertussis Specimens • Nasopharyngeal (NP) wash or swab • Use for culture, PCR • Throat swabs, cotton-tipped swabs not acceptable and inhibit growth of B. pertussis *A video of NP swab collection is available at: http://video.cdc.gov/asxgen/nip/isd/swabdemo.wmv Collecting NP Swabs for Pertussis Testing • Requires 2 Dacron tipped swabs with flexible shafts per patient – One placed in Regan Lowe Transport Media at bedside (used for culturing) – One placed in a sterile tube without media (used for PCR) • Avoid contamination • Failure to follow these procedures can cause – False negatives – False positives Antibiotic Treatment • Macrolide antibiotics first-line – 5-day course of azithromycin, or – 7-day course of clarithromycin, or – 14-day course of erythromycin • Alternative is a14-day course of TMP/SMX • Treat persons >1 year within 3 weeks of cough onset (up to 90% clear infection in 3-4 weeks) • Treat persons <1 year within 6 weeks of cough onset (infectious longer) • Postexposure antibiotics to case contacts within 3 weeks of exposure Fairfield, Lexington, Newberry, Richland 803-576-2749 Chester, Lancaster, York 803-286-9948 Reporting Pertussis to DHEC • Providers required to report – Not the sole responsibility of laboratories • Report suspected or confirmed cases – No need to wait for lab confirmation • DHEC assists providers – Diagnostic testing – Outbreak investigation and control • Identification of source cases • Contact tracing for antibiotic prophylaxis • Vaccine resources Pertussis Case Investigation • Suspect pertussis infection – Infant with: initially URI symptoms*, coughing, apnea, gagging, gasping, hypoxia, seizures; contact with a coughing individual – Older child or adult with: cough illness, paroxyms, whooping, post-tussive vomiting, prolonged cough; cases may be diagnosed with ‘bronchitis’ • Inform local DHEC county • Collect specimens – Culture and PCR (use recommended methods, materials) – Begin treatment (do not wait for lab confirmation) Pertussis Case Investigation • Identify contacts during infectious period – Most infectious at cough onset through 21 days after cough onset – Close contacts should receive antibiotic prophylaxis, regardless of vaccination • Pertussis is highly infectious • Use standard and droplet precautions – Consider face masks to all patients with URI (flu, pertussis, etc) • Cases must stay home until completion of 5 days of antibiotics Clinicians and Pertussis • Use recommended methods to diagnose and treat suspected cases – Early diagnosis and treatment will prevent infant cases and deaths • Use postpartum cocooning strategies to vaccinate parents, families of newborns before mother is discharge • Ensure patients are appropriately vaccinated with DTaP and Tdap Pertussis Vaccines: Got Tdap? Pertussis Vaccines • DTaP – Infant/childhood vaccine – Ages 6 weeks to 6 years • Tdap – Adolescent/Adult vaccine – Ages 10 to 64 years • Group in whom studies were done • No licensed vaccine for those 7-9 years of age • Some off label use reported for >64 year olds Pertussis Vaccines Ref: Sandora et al. Clin Microbiol Rev. 2008:21(3);426-434. DTaP Adverse Reactions • Local reactions • Temp of 101° or higher • More severe adverse reactions not common • Local reactions and fever more common following 4th and 5th doses (swelling involving entire thigh or upper arm has been reported—NOT a contraindication to 5th dose) DTaP Precautions • Moderate or severe acute illness • Temperature 105° (40.5° C.) or higher within 48 hours with no other identifiable cause • Collapse or shock-like state (hypotonic hyporesponsive episode) within 48 hours • Persistent, inconsolable crying lasting 3 hours or longer, occurring within 48 hours • Convulsions with or without fever occurring within 3 days DTaP/Tdap Contraindications • Severe allergic reaction (anaphylaxis) to vaccine component or following a prior dose • Encephalopathy not due to another identifiable cause occurring within 7 days after vaccination with a pertussiscontaining vaccine Tdap in Persons with Adverse Events after DTaP • Occurrence of adverse reactions (precaution) following DTaP vaccine in childhood is NOT a contraindication or precaution to administration of Tdap to an adolescent or adult Tdap Precautions • History of a severe local reaction (Arthus reaction) following a prior dose of a tetanus and/or diphtheria toxoid-containing vaccine • Progressive neurologic disorder until the condition has stabilized • History of Guillain-Barré syndrome within 6 weeks after a prior dose of tetanus toxoidcontaining vaccine • Moderate or severe acute illness Tdap Adverse Reactions • Local reactions 21%-75% (pain, redness, swelling) • Temp of 100.4oF or higher 3%-5% • Adverse reactions occur at approximately the same rate as Td alone Tdap Recommendations • Approved as a single booster to replace Td in persons fully vaccinated with pediatric DTaP or DTP Routine administration at 11-12 year well visit. Adolescents and adults <65 years of age who have not received a dose of Tdap, or for whom vaccine status is unknown, should be immunized as soon as feasible. • Priority groups Health care personnel (HCP) Any individual with infant contact (<1 year of age) • Use Tdap for wound prophylaxis, not Td, if not already received Tdap Adolescents/Adults With History of No/Unknown Tetanus, Diphtheria, or Pertussis Vaccination • All adolescents and adults should have documentation of having received a series of DTaP, DTP, DT, or Td • Persons without documentation should receive a series of 3 vaccinations • Preferred schedule: – Single dose of Tdap* – Td at least 4 weeks after the Tdap dose – Second dose of Td at least 6 months after the Td dose * If not administered as the first dose, Tdap can be substituted for any of the other doses in the series. Use of Tdap Among Pregnant Women • Td is generally preferred during pregnancy • Women who have not received Tdap should receive a dose in the immediate post-partum period • Any woman who might become pregnant is encouraged to receive a single dose of Tdap • Pregnancy is not a contraindication for Tdap • Clinician may choose to administer Tdap to a pregnant woman in certain circumstances – Such as during a community pertussis outbreak • Tdap OK for lactating women DTaP Coverage • 84.9% of children 19-35 months have received 4 or more doses of DTaP/DTP/DT • 93% DTaP coverage among children entering kindergarten for 2008-2009 school year Ref: J. Liang, Pertussis Vaccines, CDC ACIP Presentation, June 2010 Tdap coverage among adolescents 13-17 years NIS Teen, U.S. and S.C. Why aren’t More Teens Getting Vaccinated? • Many parents and students still unaware of disease, vaccine • Fewer health maintenance visits – Usually seen only when sick • Missed immunization opportunities • Episodic healthcare from healthcare providers in varied settings – Gyn offices and EDs that have rarely offered routine vaccination services to adolescents • Misperception about vaccine safety Self-reported Tdap vaccination coverage among U.S. adults – NHIS, 2008 Ref: B. Miller, Factors influencing Tdap coverage, 2010 NIC Presentation Barriers to Tdap Vaccination, Adult 2007 NIS • Low awareness of vaccine existence • Relative absence of provider recommendations • Low perceived risk among unvaccinated adults – Likely have contributed to low coverage – Despite this, many adults would be receptive to the idea of being vaccinated with Tdap, if provider recommends Ref: B. Miller, Factors influencing Tdap coverage, 2010 NIC Presentation Minimum Interval Between Tdap and Td • ACIP did not define an absolute minimum interval between Td and Tdap • Confusing language has caused providers to delay vaccination and miss opportunities to vaccinate Minimum Interval Between Tdap and Td – Removing a Barrier Tdap can be given regardless of the interval since the last Td was given. (CDC ACIP vote October 2010—expected language) – Safety data available—reduces concern for AEs due to frequent, reported exposure to antigens. – Need to improve vaccination rates and protect vulnerable infants Extending Tdap Age Indications to 7-9 Year olds • ACIP reviewed adverse event data in 4-8 year olds given Tdap in place of 5th DTaP --No increased risk of severe local or systemic adverse events compared to using DTaP 5th dose • ACIP reviewed immunogenicity data in 4-6 year olds given Tdap in place of 5th DTaP --No difference between Tdap and DTaP recipients in antibody response against pertussis antigens --Immunity similar between Tdap and DTaP recipients 3-5 years later Extending Tdap Age Indications to 7-9 Year olds • ACIP (expected) language --Children 7-10 years of age who are not fully immunized against pertussis (i.e., did not complete a series of pertussis-containing vaccine before their seventh birthday) should receive a one-time dose of Tdap. Extending Tdap Age Indications to > 65 year olds • New recommendation depends on contact with infant <12 months: (expected language from ACIP) --Full recommendation: Adults > 65 years of age who have or anticipate having contact with infants (e.g., grandparents, childcare providers, HCWs) should receive a single dose of Tdap… --Permissive recommendation: For adults > 65 years of age, a single dose of Tdap may be given… Have you received your Tdap? Questions? Resources • • • • • • • • • • DHEC pertussis site http://www.scdhec.gov/health/disease/immunization/pertussis.htm DHEC 2010 list of reportable conditions http://www.scdhec.gov/administration/library/CR-009025.pdf CDC pertussis site www.cdc.gov/pertussis CDC Recommended Antimicrobial Agents for Treatment and Postexposure Prophylaxis of Pertussis http://www.cdc.gov/mmwr/PDF/rr/rr5414.pdf CDC Prevention of Pertussis, Tetanus, and Diphtheria Among Pregnant and Postpartum Women and their Infants http://www.cdc.gov/mmwr/PDF/rr/rr5704.pdf Additional CDC pertussis vaccine recommendations http://www.cdc.gov/vaccines/pubs/ACIP-list.htm#pert CDC Pinkbook, Pertussis http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/pert.pdf Immunization Action Coalition http://www.immunize.org/pertussis/ AAP Redbook Antibiotics for Pertussis CDC. MMWR : 2005;54:14. DTaP Vaccine Efficacy • 85.2% (95% CI: 80.6 to 88.8) • 88.7% (95% CI: 76.6 to 94.6) Ref: J. Liang, Pertussis Vaccines, ACIP June 2010 Tdap Impact: Studies, Disease Rates • Based on efficacy studies before licensure – 85%-92% • Based on effectiveness studies after licensure – 66%-78% – Since Tdap licensure, pertussis rates among adolescents have declined faster compared to other age groups Ref: J. Liang, Pertussis Vaccines, ACIP June 2010 Improving Pertussis Diagnostics: Current and Future Efforts • Serologic assay kit – Revisit the CSTE case definition • Multi-target PCR assay • Pertussis Clinical Validation Study • Public health lab training – Consider testing at SC DHEC laboratory: discuss with local DHEC epis first (803576-2749) Serology Pros Cons •Can be used later in disease course •Less affected by antibiotic treatment •No standardized test •May be affected by recent immunization •Not useful during first 2 weeks of illness •Not currently included in CSTE case definition - Not counted for surveillance purposes