ACT subsidy- operational pitfalls and opportunities Chris
advertisement

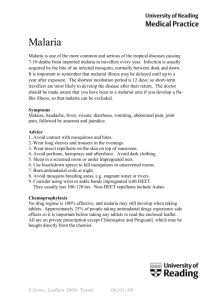
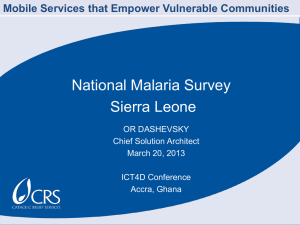
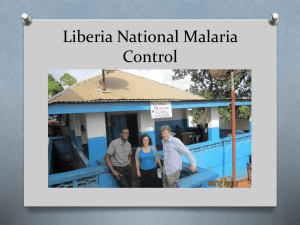
ACT subsidy- operational pitfalls and opportunities Christopher Whitty Evidence to All-Party Parliamentary Malaria Group 2007 Parasitological failure for antimalarials by day 28, Tanzania 80.0 % infections 70.0 60.0 50.0 recrudescences 40.0 new infections 30.0 20.0 10.0 AQ AQ+SP AQ+AS treatment group CoArtem Many of children with malaria come nowhere near formal healthcare Nigeria. Home 11%, traditional healer 12%, patent medicine dealer 36%, community health worker 2%, private clinic 2%, health centre 13%, hospital 4%. (Uzochukwu BS, Onwujekwe OE Int J Eq. Heal 2004) Uganda. 45% of mothers seek any care for their children with fevers (Mbonye, SciWorldJ 2003). Of those that do 53% drug vendors/shops, 31% government health facilities. (Tumwesigire & Watson. Afr Health Sci 2002) Mali. 76% mothers treat child's malaria at home (Thira et al TM&IH 2000) Kenya. Only 32% of patients with fevers made at least one visit to a health care facility. (Guyatt & Snow Trans RSMH 2004) Indirect cost of care is the major barrier to accessing formal healthcare, then transport • Over half of the cost of a treatment episode is indirect cost (Wiseman et al PLOS Medicine 2006) • Opportunity cost, childcare, transport, information all barriers • The poorest will go to the closest care. • This will almost always be the private sector. Ability and willingness to pay • Tanga region- average person gets malaria 3-5x a year • May have 10 people dependent on a single income of $20 a month • Cost of ACTs in the market $711 • Willingness to pay for ACT at public health facilities- $0.8 (Wiseman et al, Bull WHO) Fake drugs and Veblen goods- further reasons the price of ACTs in the private sector must come down (Newton et al PLoS Medicine 2006; CDC warning sheet 2006) Those involved in antimalarial drugs policy have sometimes made optimistic economic assumptions. • “If the quantity [of a good] should …fall short of the effectual demand… its price must rise” (Adam Smith, 1776) • “As orders for the drug increase, the price of ACT will go down” (ACT Now Campaign 2003) • “[it’s] created a major wave of shock in our organization ” RBM spokesman, NY Times 14/11/2004 when 6 months after almost every country in Africa adopted ACTs as policy simultaneously the price of raw material quadrupled Can we leave it to the market? • Limited range of competitors- but this is improving • Substitution cost- alternative cash crops, high barriers to entry- cost of chemical plant for extraction. We are paying for risk and inefficiency. • Immature market; poor demand and supply forecasting. • Possibility of synthetics makes return on capital uncertain. • Shelf-life short- need good stock control or significant wastage. • Price elasticity not certain- but non-linear Access is one problem, which the subsidy will help with. Overprescription is another. Need malaria treatment Receive malaria treatment Over-diagnosis of malaria- a major problem Syndromic management without tests common. Where microscopy available negative tests widely ignored. Between 30% and 99% of those prescribed antimalarials do not have malaria parasites Cost-effectiveness of ACTs falls rapidly as misdiagnosis occurs. Serious alternative diagnoses missed. Prescription does not change with changing risk. Tanzania- ratio treated with positive test to negative test 1:3 (Reyburn et al BMJ) Febrile patients recruited 2,416 Blood slide 1,214 RDT 1,202 Positive 174 (14%) Negative 1,031 (86%) Positive 190 (16%) Negative 1,008 (84%) Antimalarial 171 (98%) Antimalarial 523 (51%) Antimalarial 188 (99%) Antimalarial 543 (54%) Low transmission ratio treated with positive test : negative test 1:116 (Reyburn) Recruited 824 RDT 406 Blood slide 418 Positive 1 Negative 417 Positive 3 Antimalarial 1 Antimalarial 227 (54%) Antimalarial 3 Negative 403 Antimalarial 235 (58%) Over-diagnosis of malaria is a threat, but also an opportunity • We have to accept that there will be waste of drugs- there already is. • The worst that can happen is that the situation starts bad and stays bad • It is more likely that the situation starts bad and gets better. • This could have an impact not just on malaria, but on the other causes of febrile illness- which also kill children. There is a realistic hope for artemisinins to come down in price in the medium term What evidence there is suggests a reduction of malaria, and certainly not an increase • Good evidence from South Africa, Zanzibar • Indirect evidence from Tanzania, Gambia, Kenya, Uganda • Major impact in some areas from PMI, and long lasting ITNs There are reasonable grounds for thinking a subsidy is necessary, and would taper down over time. ACTs are needed, they need to be provided outside the formal sector, including the private sector, and the market will not in itself get the prices low enough to achieve this. • We have to accept there will be waste, and this will be slow to correct. • All the long term trends are likely to favour the subsidy tapering away, including -greater competition with more ACTs -new sources of raw product, and reduction in risk pricing (-probably reduction in overprescription and in malaria incidence reducing demand)