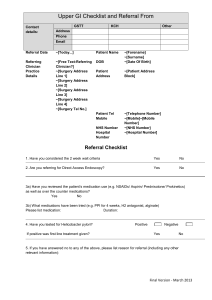
Dysphagia, GERD, H pylori - UNM Internal Medicine Resident Wiki

Upper GI potpourri
Anthony Worsham, MD
Division of Hospital Medicine
Department of Internal Medicine
University of New Mexico Health Sciences Center
Thursday, October 9, 2014
Outline
● dyspepsia
● gastroesophageal reflux disease (GERD)
● peptic ulcer disease
●
Barrett’s esophagus
●
Helicobacter pylori
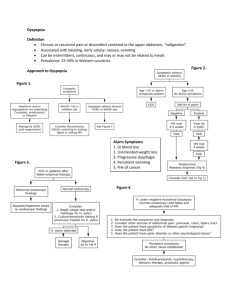
What is dyspepsia?
Functional dyspepsia
“presence of symptoms thought to originate in the gastroduodenal region, in the absence of any organic, systemic, or metabolic disease”
Rome III diagnostic criteria (at least 1 of)
Bothersome postprandial fullness
Early satiation
Epigastric pain
Epigastric burning
No evidence of structural disease
Functional dyspepsia
Differential diagnosis
Functional (nonulcer) dyspepsia
Peptic ulcer disease
Reflux esophagitis
Gastric or esophageal cancer
Abdominal cancer, especially pancreatic cancer
Biliary tract disease
Carbohydrate malabsorption (lactose, sorbitol, fructose, mannitol)
Gastroparesis
Hepatoma
Infiltrative diseases of the stomach (Crohn disease, sarcoidosis)
Intestinal parasites (Giardia species, Strongyloides species)
Ischemic bowel disease
Medication effects (Table 3)
Metabolic disturbances (hypercalcemia, hyperkalemia)
Pancreatitis
Systemic disorders (diabetes mellitus, thyroid and parathyroid disorders, connective tissue disease) Rare
Loyd RA and McClellan DA. Update on the evaluation and management of functional dyspepsia. Am Fam Physician
2011; 83(5): 547-552
Up to 70 percent
15 to 25 percent
5 to 15 percent
< 2 percent
Rare
Rare
Rare
Rare
Rare
Rare
Rare
Rare
Rare
Rare
Rare
●
Upper gastrointestinal alarm symptoms
Age ≥55 years with new onset dyspepsia
●
Chronic gastrointestinal bleeding
●
Dysphagia
●
Progressive unintentional weight loss
●
Persistent vomiting
●
Iron deficiency anaemia
●
Epigastric mass
●
Suspicious barium meal result taken from National Institute for Health and Care (formerly Clinical) Excellence referral guidelines for suspected cancer
Functional dyspepsia treatment
Diet and lifestyle
–
–
– weight loss smoking and alcohol cessation
Avoid certain foods (e.g., fatty foods)
Medication
–
–
–
– acid suppression therapy (e.g., PPIs)
H. pylori eradication therapy prokinetic drugs (e.g., metoclopramide, cisapride, domperidone) antidepressants and psychologic therapies
Alternative therapies (e.g., accupuncture)
Ford AC. Dyspepsia. BMJ 2013;347:f5059
What is GERD?
Definition
“GERD should be defined as symptoms or complications resulting from the reflux of gastric contents into the esophagus or beyond, into the oral cavity (including larynx) or lung. GERD can be further classified as the presence of symptoms without erosions on endoscopic examination (nonerosive disease or NERD) or
GERD symptoms with erosions present (ERD).”
Katz et al, Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol
Kahrilas PJ, Boeckxstaens G. Failure of reflux inhibitors in clinical trials: bad drugs or wrong patients? Gut 2012;61:1501 –1509.
Kahrilas PJ, Boeckxstaens G. Failure of reflux inhibitors in clinical trials: bad drugs or wrong patients? Gut 2012;61:1501 –1509.
GERD treatments
● lifestyle modification
● medication
● surgery
Kahrilas PJ, Boeckxstaens G. Failure of reflux inhibitors in clinical trials: bad drugs or wrong patients? Gut 2012;61:1501 –1509.
Top 100 Most Prescribed, Top Selling Drugs.
http://www.medscape.com/viewarticle/825053
PPI Complications
● community-acquired pneumonia
● hip fracture
● infectious gastroenteritis
●
C difficile
●
Vitamin B12 deficiency/malabsorption
● secondary hypergastrinemia
● hypochlorhydria
Kahrilas PJ, Gastroesophageal reflux disease, NEJM 2008;359:1700-7.
Katz et al, Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013; 108:308
Peptic ulcers can be deadly
Rudyard Kipling J. R. R. Tolkien James Joyce
Ulcer complications
● bleeding
● perforation
● penetration
Management of acute bleeding from a peptic ulcer
Clinical status
●
At presentation
Assess hemodynamic status (pulse and blood pressure, including orthostatic
●
●
●
● changes).
Obtain complete blood count, levels of electrolytes (including blood urea nitrogen and creatinine), international normalized ratio, blood type, and cross-match.
Initiate resuscitation (crystalloids and blood products, if indicated) and use of supplemental oxygen.
Consider nasogastric-tube placement and aspiration; no role for occult-blood testing of aspirate.
Consider initiating treatment with an intravenous proton-pump inhibitor (80-mg bolus dose plus continuous infusion at 8 mg per hour) while awaiting early endoscopy; no role for H2 blocker.†
●
●
Perform early endoscopy (within 24 hours after presentation).
Consider giving a single 250-mg intravenous dose of erythromycin 30 to 60 minutes before endoscopy.
●
Perform risk stratification; consider the use of a scoring tool (e.g., Blatchford score16 or clinical Rockall score17) before endoscopy.
At early endoscopy
Perform risk stratification; consider the use of a validated scoring tool (e.g., complete
Rockall score17) after endoscopy.
Low-risk lesions
Gralnek IM, et al. Management of acute bleeding from a peptic ulcer. NEJM 2008;359:928-37
Recommended treatment to prevent ulcer rebleeding
Laine L and Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol 2012; 107:345
–360;
Peptic ulcer treatment
All NSAIDs are associated with GI bleed
Barrett’s esophagus
Spechler SJ and Souza RF. Barrett’s esophagus. N Engl J Med 2014;371:836-45.
Helicobacter pylori
H . pylori treatment regimens
Triple therapy (7-14 days)
– PPI, healing dose bid
– amoxicillin 1 gm bid
– clarithromycin 500 mg bid
Sequential therapy
– Days 1-5
–
●
●
PPI, healing dose bid amoxicillin 1 gm bid
Days 6-10
●
●
●
PPI, healing dose bid clarithromycin 500 mg bid tinidazole 500 mg bid
Quadruple therapy
– PPI, healing dose bid
– tripotassium dicitratobismuthate, 120 mg qid
– tetracycline 500 mg qid
– metronidazole 250 mg qid
Healing dose PPI (all bid)
– omeprazole 20 mg
– pantoprazole 40 mg
– lansoprazole 30 mg
– esomeprazole 20 mg
H. pylori testing
Testing criteria
●
Active gastric or duodenal ulcer
● history of active gastric or duodenal ulcer not previously treated for H. pylori infection
● gastric MALT lymphoma
● history of endoscopic resection of early gastric cancer
● uninvestigated dyspepsia
Test-and-treat criteria
● age <55 yr and no alarm symptoms