Comparing “Vaginal Infection” as Chief Complaint to Subsequent Treatment at a Clinic in Rural Haiti
World Health Student Organization
John Dawdy1; Dr. Jeffrey Van Laere, M.D.2; Justin Gerard1; Priyanka Singh1; Terrie Ahn1; Dr. Diane Levine, M.D.3
1Wayne State University School of Medicine; Detroit Medical Center, 2Department of Emergency Medicine and 3Department of Internal Medicine
INTRODUCTION
METHODS
DISCUSSION
Sexually transmitted infections are among the most common infectious diseases,
and make significant contributions toward morbidity and mortality in developing nations. If
left untreated, these infections contribute to reproductive morbidity and mortality, adverse
pregnancy outcomes, and enhanced acquisition or transmission of HIV infection.
An interdisciplinary health care team of physicians, students and pharmacists from
the Wayne State University School of Medicine traveled to Haiti to operate a 5 day long
medical clinic in March of 2014. The clinic was located in Morne de l’Hopital, a rural
community in the mountainous area outside of Port-au-Prince.
An impoverished nation already, the earthquake that hit Haiti in 2010 led to the
collapse of an already fragile social, economic and health infrastructure that has been
slow to recover. The limited financial resources, social infrastructure, community health
networks, and significant stigma surrounding STIs are particularly important roadblocks to
proper education, diagnosis and treatment.
Each patient that attended the clinic had an associated patient intake form where
demographic information, symptoms, history of present illness, diagnosis, and treatment
were recorded. Patient intake forms from the clinic were reviewed for chief complaints
related to vaginal infection along with subsequent diagnoses and treatment plan.
The dire consequences associated with these infections and the poverty of
resources available to local health workers has led public health organizations, including
the WHO and Haiti’s Ministry of Health, to promote the use of a syndromatic approach to
treatment. As such, all patients that present with symptoms associated with an STI are
treated empirically. This form of approach has been shown to have both low sensitivity
and specificity.
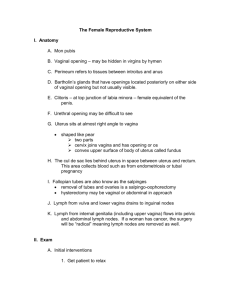
Figure 1. Protocol
for treatment of
vaginal discharge
and/or itchiness
among women in
Haiti, Ministry of
Health
Woman presents with vaginal discharge and/or
itchiness
If vaginal ulcerations are present, treat using
appropriate algorithm
Ask patient if partner has symptoms of STIs (urethral
discharge, pain/burning upon urination)
Yes
No
Screen for the following risk factors:
• Age <21 years
• Living alone/not living with partner
• >1 sexual partner during the past 6 months
• New sexual partner during the past 3 months
Diagnosis used a heavily syndromatic approach, based predominantly on clinical
presentation and limited diagnostic tools to rule out other possible diagnoses. Tools used
were:
1) History: pertinent positives included pain or burning with urination, changes in vaginal
discharge, a sexual partner with a STI, lower abdominal pain, or pain/bleeding during
sexual intercourse.
2) Physical exam, including speculum exam: pertinent positives included purulent vaginal
or cervical discharge, vaginal bleeding outside of menstruation, cervical friability,
cervical motion tenderness, or lower abdominal tenderness.
3) pH test strips and the Whiff test: used to rule out bacterial vaginosis.
4) Urinalysis: performed to rule out urinary tract infection.
RESULTS
Increased antibiotic resistance is often a key talking point for advocates of reducing
such overtreatment, and it also appears that significant resources could be saved within a
health system that is already strained. When you also consider patient reassurance that
what they are experiencing is normal, a more educated patient population with regards to
vaginal discharge offers a number of clear benefits.
Diagnosis
Vaginal Symptoms
70
30
65
24
25
<2 risk factors
50
47
20
•Treat patient for cervical infection and vaginitis
•Provide counseling, education, and condoms to patient and
partner(s)
•Emphasize importance of taking all medications
•Treat partner(s) for STIs
•Reassess if no improvement in symptoms after 15 days
This knowledge deficit suggests that educational initiatives that not only address
common causes of vaginitis and STI prevention but also include education regarding the
normal discharge experienced by women could be beneficial for this and other similar
communities. Our trip included a partnership with a local nurse to lead education sessions
for patients in Creole. Similar community-based approaches to patient education have
proved successful in the past, and including this often neglected topic within these
initiatives could begin to fight the culture of overtreating vaginal discharge.
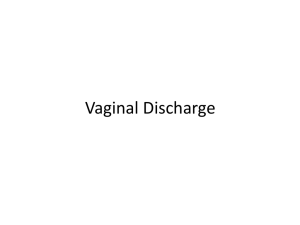
Of 304 female patients that attended the clinic, a total of 92 patients presented with a chief
complaint of “vaginal infection”. From these 92 patients, 51 were treated for such
infections.
60
>2 risk factors
Based on our experience, it appears that patients often misinterpret the clinical
signs and symptoms of a vaginal discharge. Interactions with patients that attended this
clinic would suggest that there is a general awareness of STIs in the community. However,
a more comprehensive women’s health education would be beneficial in improving
understanding of variability of normal vaginal discharge. Experiences with past medical
mission trips that have used empiric treatment of vaginal discharge has contributed to the
medicalization of discharge and a perception that all instances require pharmacologic
treatment. This not only leads to an expectation of treatment when attending clinics, but
results in patient reporting self-treatment with available antibiotics when access to clinics
is not available.
18
39
40
18
REFERENCES
15
•Treat for vaginitis
•Provide counseling, education, and
condoms to patient and partner(s)
30
19
20
10
10
14
6
10
AIM
We looked at the prevalence of “vaginal infection” as a chief complaint at a clinic in
rural Haiti and compared it to the number of patients that were subsequently treated for
this complaint. It is suspected that many patients lack adequate knowledge of normal
vaginal discharge and the variation of discharge during the menstrual cycle, leading to an
overestimation of its prevalence within the patient population.
7
5
5
1.
5
1
0
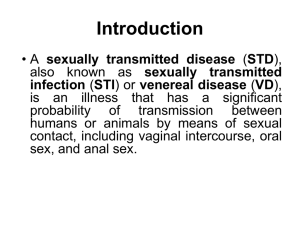
Burning with Discharge
urination
Frequency
Itching
Odor
Pain
Pain with
Sex
Figure 2 . Number of patients presenting with
common vaginal symptoms
0
Atrophic
Vaginitis
Bacterial
Vaginosis
STI
UTI
Vaginal
Infection
Yeast
Infection
Normal
Vaginal
Discharge
Figure 3 . Diagnosis of patients that presented
with “vaginal infection”
2.
3.
Smith Fawzi MC, Lambert W, Singler J, et al. Identification of chlamydia and
gonorrhoea among women in rural Haiti: maximising access to treatment in a
resource poor setting. Sex Transm Infect 2006; 82: 175-181.
Logie CH, Daniel C, Newman PA, Loutfy MR. An HIV/STI prevention intervention for
internally displaced women in Leogane, Haiti: study protocol for an N-of-1 pilot
study. BMJ Open. 2012; 2:e001634
Centers for Disease Control and Prevention. Sexually Transmitted Infections in
Developing Countries. Atlanta: U.S. Department of Health and Human Services;
2008.