Obstetric Emergencies
Postpartum Hemorrhage and Hypertension
Annelee Boyle, MD, FACOG
Assistant Professor
Department of Obstetrics and Gynecology
Division of Maternal-Fetal Medicine
University of Virginia School of Medicine
Disclosures
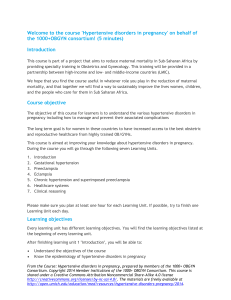
Pregnancy-related mortality in the United States: 1987-2010
Source: CDC Pregnancy Mortality Surveillance System
Obstetrics and Gynecology, May 2014
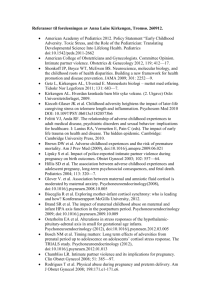
Causes of pregnancy-related death in the United States: 2006 -2010
Source: CDC Pregnancy Mortality Surveillance System
Maternal mortality is only the tip of the iceberg
Obstetrics and Gynecology, February 2012
Postpartum Hemorrhage
•
93% of deaths preventable!
–
•
Berg et al. Preventability of pregnancy related deaths: results of a statewide review.
Obstet Gynecol 2005; 106:1228-34.
Common mistakes:
– Under-recognition of blood loss
– Under-recognition of hypovolemia
– Failure to act decisively
– Failure to restore blood volume
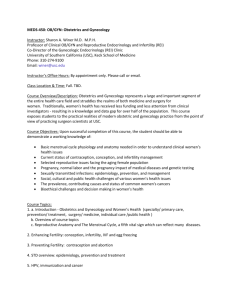
Recognize the extent of blood loss
Dildy et al, Estimating Blood Loss: Can Teaching Significantly Improve Visual
Estimation? Obstetrics & Gynecology. 104(3):601-606, September 2004.
Recognize the extent of hypovolemia
Class 1
< 750ml
Class 2
Class 3
EBL in ml
750-1500ml 15002000ml
EBL in % Vol. <15%
15-30%
30-40%
Pulse
<100
>100
>120
BP
Normal or ↑ ↓
↓
RR
14-20
20-30
30-40
UOP
>30ml/h
20-30ml/h 5-15ml/h
Mental
Slightly
Mildly
Anxious,
State
anxious
anxious
confused
Class 4
>2000ml
>40%
>140
↓
>35
negligible
Confused,
lethargic
Obstetrics and Gynecology, May 2014
Early warning signs
•
•
•
•
•
•
•
•
Systolic BP <90 or >160
Diastolic BP >100
Heart Rate <50 or >120
Resp Rate <10 or >30
Oxygen Sat <95% on room air
Urine output <35ml/hr for 2 hours
Agitation, confusion, or unresponsiveness
Shortness of breath or a non-remitting headache in a
patient with pre-eclampsia
– Mhyre et al. The maternal early warning criteria: a proposal from the
national partnership for maternal safety. Obstet Gynecol
2014;124:782-6.
Act decisively/Restore blood volume
Post-Partum Hemorrhage
•
Rule number one: Postpartum Hemorrhage is a definition,
not a diagnosis!
Pearls for Atony
•
Actively manage the third stage of labor
Pearls for Atony
•
Consider additional utero-tonics for those at highest risk of
PPH
Pearls for Lacerations
•
Have a low threshold for going to the OR for repair.
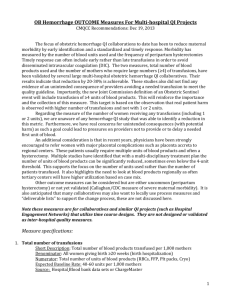
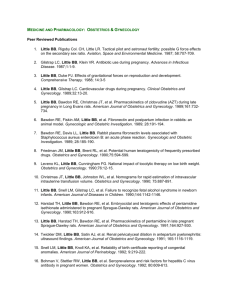
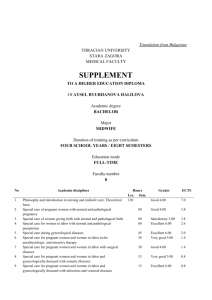
Risk of accreta in the setting of placenta previa by
number of prior cesareans
80%
70%
60%
50%
40%
30%
20%
10%
0%
No prior CD
1
2
3
4 or more
Source: California
Maternal Quality
Care Collaborative
Preelcampsia
•
60% of deaths are preventable!
–
•
Berg et al. Preventability of pregnancy related deaths: results of a statewide review.
Obstet Gynecol 2005; 106:1228-34.
Common mistakes:
– Failure to adequately control blood pressure
– Failure to recognize HELLP syndrome
– Failure to diagnose and treat pulmonary
edema
Early warning signs
•
•
•
•
•
•
•
•
Systolic BP <90 or >160
Diastolic BP >100
Heart Rate <50 or >120
Resp Rate <10 or >30
Oxygen Sat <95% on room air
Urine output <35ml/hr for 2 hours
Agitation, confusion, or unresponsiveness
Shortness of breath or a non-remitting headache in a
patient with pre-eclampsia
– Mhyre et al. The maternal early warning criteria: a proposal from the
national partnership for maternal safety. Obstet Gynecol
2014;124:782-6.
Control Blood Pressure
Control Blood Pressure
Hi Annelee. Hope you’re doing well and liking your new
job. It’s 10:30 pm here and for me, that’s the middle of the
night so rather than be friendly and “chat”, I’m going to get
straight to the point – it’s business…
So our hospital protocol essentially regurgitates ACOG, but it
doesn’t specify that it is for use only with
preeclamptic/eclampic patients. Would you use it for someone
with chronic HTN also, barring known renal disease or other
cause of the HTN?
Thanks!
Love, Aunt Crunchy
Recognize HELLP Syndrome
The most important paper on HTN in pregnancy
in the last year
Severe Features of Preeclampsia
•
•
•
•
•
•
•
•
SBP >160
DBP >110
Platelets < 100,000)
LFTs >2x normal
Creatinine > 1.1
Pulmonary edema
New-onset cerebral or visual disturbances
Right upper quadrant pain
American College of Obstetricians and Gynecologists. Hypertension in
pregnancy: executive summary. Obstet Gynecol 2013;122:1122–31.
Recognize and treat pulmonary edema
The UVA way (or maybe it was UNC)
“If you’re going
down take
everybody else
with you.”
– Susan Modesitt, Gyn Oncologist
David Barker 1938-2013
The Barker Hypothesis
The Thrifty Phenotype
Fetal Origins Hypothesis
Intrauterine Growth Restriction
30 years from now
Thank you!!!