Diapositiva 1
advertisement

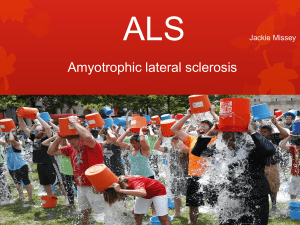
COMORBIDITIES IN ALS PATIENTS FROM EMILIA ROMAGNA: A POPULATION BASED STUDY. J. Mandrioli, N. Fini, E. Georgoulopoulou, S. Biguzzi, E. Venturini, C. Guidi, E. Sette, E. Terlizzi, A. Ravasio, M. Casmiro, F. Salvi, R. Liguori, R. Rizzi, V. Pietrini, E. Chierici, M. Santangelo, E. Granieri, V. Mussuto, A. Borghi, R. Rinaldi, S. De Pasqua, R. D’Alessandro and ERRALS Group. Neurological Departments of Modena, Cesena, Forlì, Ferrara, Piacenza, Rimini, Ravenna, Bologna, Reggio Emilia, Parma, Fidenza, Carpi, Imola INTRODUCTION There have been few studies of comorbidities among patients with ALS, reporting contrasting results on cardiovascular, autoimmune, metabolic or neurological diseases (1). Among clinicians, there is a general perception that patients with ALS can be premorbidly healthier than the general population, and previous papers reported an increased risk of ALS among people doing professional physical activity (2), with a lower body mass index (3), and reduced cardiovascular risk (4). We performed a population-based study in Emilia Romagna Region focusing on ALS comorbidities. METHODS From 2009 onwards, a prospective registry, involving 9 provinces has been collecting all cases of incident ALS among residents in Emilia Romagna region (population 4.4 million inhabitants). For each patient, the main demographic and clinical information, including comorbidities, were collected by the caring physicians and input in a dedicated website at diagnosis. RESULTS From 1.1.2009 to 31.12.2013 in Emilia Romagna newly diagnosed ALS patients were 566 (M/F: 1.2; mean age at onset: 66.4 years). Patients with a history of chronic/ongoing diseases were 445 (78.6%): 247 (55.0%) had hypertension, 76 (17.07%) heart diseases, 57 (12.81%) neoplasms, 55 (12.36%) thyroid disorders, 50 (11.24%) diabetes, 50 (11.24%) chronic obstructive pulmonary disease (COPD), 39 (8.76%) dyslipidemia, 29 depression (6.52%), 26 (5.84%) cerebrovascular diseases, 23 (5.17%) rheumatic diseases. Among neurological diseases: 46 (10.33%) dementia, 12 (2.70%) Parkinson’s Disease, 5 (1.12%) epilepsy, 2 (0.45%) mental retardation, only 1 case of myasthenia, and 1 case of multiple sclerosis were observed. Patients with comorbidities were older (68 vs 60 yrs at onset, p<0.01), more often with bulbar onset (39.55% vs 21.49%, p<0.01). Flail phenotypes were more often represented among patients without comorbidities; the opposite for respiratory and bulbar phenotype. At univariate analysis patients with comorbidities had an HR of 1.34 (p=0.03), but at multivariate analysis disease duration was not significnatly different between patients having comorbidities or not. 1.00 0.75 14.22 60.28 26 (21.49%) 95 (78.51%) 28 (23.14%) 54 (44.62%) 31 (25.6%) 6 (4.95%) >4 diseases 5.6% 4 diseases 12.5% No comorbidities 21.4% no comorbidities 1 disease 0.50 12.55 68.11 176 (39.55%) 269 (60.35%) 165 (37.07%) 186 (41.79%) 73 (16.40%) 21 (4.72%) N. of diseases Survival estimates by comorbidities 2 diseases 3 diseases 15.7% 1 disease 20.1% 0.25 No comorbidities 70/51; 1.37 2 diseases 24.6% 0.00 sex (M/F; ratio) onset-diagnosis (months) age at onset bulbar onset spinal onset bulbar phenotype classic phenotype flail phenotype UMNp phenotype Respiratory phenotype Comorbidities 242/203; 1.19 0 12 24 36 48 60 72 84 96 108 120 132 3 diseases 4 diseases >4 diseases 144 survival from onset (months) 17 (3.82%) 2 (1.65%) no comorbidities comorbidities DISCUSSION Patients with ALS had great comorbidities with hypertension, diabetes, neoplasm, heart diseases, COPD, and thyroid disorders, as expected from a population with a mean age at onset of 66 years. The presence of these diseases does not modify disease progression and survival in patients with ALS. We confirm existing data on neurological comorbidities in ALS. Some relatively common diseases seem to be relatively less represented in our ALS cohort (e.g. dyslipidemia) but a possible role of these diseases as protective factors should be examined through ad hoc studies. References 1. Turner MR, Goldacre R, Ramagopalan S, Talbot K, Goldacre MJ. Autoimmune disease preceding amyotrophic lateral sclerosis: an epidemiologic study. Neurology. 2013;81(14):1222-5. 2. Chio A, Benzi G, Dossena M, Mutani R, Mora G. Severely increased risk of amyotrophic lateral sclerosis among Italian professional football players. Brain 2005;128(pt 3):472–476. 3. Gallo V, Wark PA, Jenab M, et al. Prediagnostic body fat and risk of death from amyotrophic lateral sclerosis: the EPIC cohort. Neurology 2013;80:829–838. 4. Turner MR, Wotton C, Talbot K, Goldacre MJ. Cardiovascular fitness as a risk factor for amyotrophic lateral sclerosis: indirect evidence from record linkage study. J Neurol Neurosurg Psychiatry 2012;83:395–398. ERRALS Group: Bologna: F. Salvi, I. Bartolomei, R. Michelucci; P. Avoni, S. DePasqua, R. Liguori; A. Borghi, A. Gabellini, T. Sacquegna; R. Rinaldi, F Cirignotta; R. D’Alessandro; Carpi: M. Santangelo, S. Amidei, G. Greco; Cesena: S. Biguzzi, E. Venturini, M.G. Passarin; Faenza and Ravenna: M. Casmiro,F. Rasi; Ferrara: E. Sette, V. Tugnoli, M.R. Tola, I. Casetta, E. Groppo, E. Granieri; Fidenza : E. Chierici, E. Montanari; Forlì: C. Guidi, W. Neri; Imola: P. De Massis, V. Mussuto; Modena: J. Mandrioli, N. Fini, E. Georgoulopoulou, P. Nichelli; Parma: A. Grassi, L. Delay, M. Aiello, V. Pietrini; Piacenza: E. Terlizzi, D. Guidetti; Reggio Emilia: R. Rizzi, E. Canali, N. Marcello; Rimini: M. Currò Dossi, M. Pasquinelli, J. Andruccioli, A. Ravasio; Department of Hospital Services, Emilia Romagna Regional Health Authority, Bologna: S. Ferro XLV CONGRESSO NAZIONALE 11-14 ottobre 2014 – CAGLIARI 415