May 3, 2013 - Kyle Carpenter
advertisement

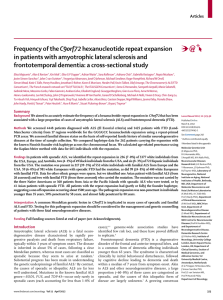
Neurology Case Kyle Carpenter PGY III History of Present Illness 60 year old left handed male Chief complaint- difficult speaking, frequent falls On his first visit his wife noted that for past 2 years the patient’s language and vocabulary had suffered He was having trouble recalling words that he wanted to say e.g. he was formerly a mechanic and was having trouble remembering names of tools His short term memory had also progressively worsened during this same time Also for about one year prior had been falling frequently (12 times per week) Difficulty swallowing and crying spells for no apparent He was no longer paying bills or driving Past medical history Hypertension Diabetes (A1C of 8.9%) Hyperlipidemia GERD Depression Social Stopped smoking and drinking 20 years prior Surgery CTS in 2011 Kidney stone Exam Mental status Can name correct city, and year but not month or day Naming intact. 2/3 object at 5min recall Comprehension intact but perseverates Speech Fluent but with severe word finding difficulty Only 8 objects on “D” test (12 is normal) Decreased emotion in speech Cranial Nerves Intact Orbicularis oculi 5/5 Tongue strength is normal Exam Motor • • Tone is normal Atrophy of FDI Right NF NE 3+ Patella Downgoing toes Gait 5 44 5 5 5 5 HF 4+ 4+ HE KF KE DF PF 4+ 4+ 5 5 4 5 3+ in bilaterally UE 0 Ankle Left 5 SA EF EE WF WE Reflexes Wide based, slow, unable to walk heel to toe 5 5 5 5 Cerebellar FNF intact but slo Sensory Difficult to assess but likely intact to all modalities 5 5 4 5 Second Visit CT head showed moderate cortical atrophy Seen in clinic three months later Almost completely anomic. 1-2 words at the most Unable to answer orientation questions Could follow 1 step commands but nothing more complicated Confined to a wheelchair, diffuse weakness Further atrophy of hands, arms, legs Fasciculations seen in leg and arm muscles Further testing was done Where? What? Frontotemporal Dementia and Amyotrophic Lateral Sclerosis FTD-ALS Each disease is typically diagnosed separately 15% of ALS patients have FTD 10% of FTD patients Slightly more common in men than women Cognitive symptoms typically occur first but motor symptoms can occur before or simultaneously Interval is 3 months to 7 years with mean of 2 years Survival is worse in FTD-ALS patients than ALS without dementia A proposed classification scheme ALSci (cognitively impaired) ALSbi (behaviorally impaired) ALS-FTD (meet Neary Criteria) FTD-MND (patients who have motor neuron loss at autopsy but no clinical signs) ALS-dementia (Alzheimer's or vascular) M. J. Strong, G. M. Grace, M. Freedman, et al., “Consensus criteria for the diagnosis of frontotemporal cognitive and behavioural syndromes in amyotrophic lateral sclerosis,”Amyotrophic Lateral Sclerosis, vol. 10, no. 4, pp. 131–146, 2009. Amyotrophic Lateral Sclerosis ALS used interchangeably with ‘Motor Neuron Disease’ and ‘Lou Gehrig's Disease’ Diagnosed clinically with a mixture of upper motor neuron signs and lower motor neuron signs Progressive weakness that can begin in legs, arms or bulbar region Atrophy and fasciculation (LMN) Hyperreflexia, upgoing toes, jaw jerk (UMN) EMG shows active denervation and reinnervation First described in 1869 by Charcot Marie in 1892 reported on behavioral changes in ALS patients Entrenched in Neurology that body wasted and mind was spared In late 80s Stan Appel and Forbes Norris developed clinics devoted to ALS clinics This concept spread to major centers allowing Neurologists to develop large ALS patient populations Reports were generated linking ALS and dementia Criteria for FTD were published in 1998 and ALS and FTD were linked FRONTOTEMPORAL DEMENTIA Symptoms Insidious onset with slow progression Age 50-60 Types Behavioral variant (bvFTD) Disinhibition, apathy, behavior changes (next slide) Primary Progressive Aphasia Decreased expression of language, anomia Relative preservation of comprehension Semantic Dementia (now considered a variant of PPA) Fluent grammatically correct speech but empty of content Loss of executive function early is seen in all three Typically preservation of short term memory, praxis and visualospatial skills Diagnosed via Neary Criteria (other criteria have been suggested) Table 1: Behavioral features in FTLD Disinhibited type Increased interest in sexual activity Lack of judgment Swearing Violation of personal space Impulsive buying Paranoia Criminal activity Grandiose thinking Ignoring social etiquette Apathetic type Blunted emotions Disinterested and withdrawn Lack of attention to personal hygiene Lack of empathy Stereotypical type Hoarding Food fads, overeating Ritualistic/repetitive behavior Testing FTD in ALS patients Can be difficult to test for language disorders due to bulbar weakness (dysarthria), hand weakness impairs writing Cognitive changes can be seen in patients follows in specialty clinics Comprehension in pulmonary testing Spelling and grammatical errors Various studies and questionnaires have used to identify dementia in ALS patients CANTABCambridge CANTAB Neuropsychological Test Automated Computer touch screen and Neurologist opinion Battery Memory loss 7%, FTD criteria 22% NPI- Neuropsychiatric Inventory Caregiver questionnaire Inventory FBIFrontal Behavioral CBI- Cambridge Behavioral Inventory NPI, FBI, CBI, FrSBe FrSBe- Frontal Systems Behavioral Apathy 56%, stereotypical behaviors 20%, executive dysfunction Scale 34-48%, disinhibition 18-27% 11% meet criteria for FTD MMSE- Mini mental Status Exam FTD In ALS 2003 study of 100 patients screened with verbal fluency and MMSE 31 had abnormal fluency (“D” or animal test). 50% of bulbar onset patients had abnormal exam, 25% of limb onset patients All had normal MMSE 2012 study of 160 patients with formal neuropsych testing 14% met FTD-Neary criteria, 21% had cognitive impairment and 47% were normal 2005 study of 279 patients 15% with FTD, 49% normal cognition, 43% cognitive impairment ALS patients over time 52 patients every 4 months showed abnormal at onset did not show decline FTD in ALS 2009 AAN practice parameter acknowledged lack of consensus of screening tool ALS Cognitive Behavioral Screen- has been validated 15 caregiver questions 8 item physician assessment 5 min Penn State Screen Battery of Frontal and Temporal Dysfunction Syndrome 20 minutes Not validated UCSF Screen Battery 45 minutes, includes ALS specific FBI and depression screen ALS in FTD patients Studies have had varied results 2002 study of 36 FTD patients with detailed neuromuscular exam and EMG 5 had definite ALS, 5 had fasciculations on EMG and 1 of these developed definite ALS 1 year later 2008 retrospective study of FTDbv 18 of 61 developed definite ALS Genetics Various genetic mutations have been linked to both familial ALS and FTD Familial cases are far outnumbered by sporadic cases in both disorders (10% of ALS and 40% of FTD) Three most important genes associated with FTD are microtubule associated protein tau (MAPT), progranulin and C9ORF72 Mutations in the SOD1 gene are most common in familial ALS Two studies in 2012 found a mutation in the C9ORF72 gene that occurred in both ALS and FTD. This was the first genetic link between the two diseases Progranulin and C9ORF72 mutations can deposition of TAR-DNA binding protein 43 (TDP-43) TDP-43 is an ubiquinated protein that has been found to accumulate in both ALS and FTD Sources ALS and Frontotemporal Dysfunction: A Review. Eugene Y. Achi and Stacy A. Rudnicki Neurology Research International Volume 2012 (2012), Article ID 806306, 9 pages doi:10.1155/2012/806306 Renton AE, Majounie E, Waite A, et al. A hexanucleotide repeat expansion in C9ORF72 is the cause of chromosome 9p21-linked ALS-FTD. Neuron 2011;72:257–268 Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 2011;134(pt 9):2456Y2477 M. J. Strong, G. M. Grace, M. Freedman, et al., “Consensus criteria for the diagnosis of frontotemporal cognitive and behavioural syndromes in amyotrophic lateral sclerosis,”Amyotrophic Lateral Sclerosis, vol. 10, no. 4, pp. 131–146, 2009.