Lecture 02 – Enterobius vermicularis
advertisement

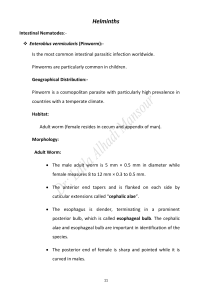
Nematodes (Round worms) General properties a. Morphology and anatomy. Nematodes have an anterior mouth and posterior anus and range from 90 µm to 1000 mm in length. They are cylindrical with a thick surface tegument; their shape is maintained by a positive hydrostatic pressure that limits movement to a sinusoidal snake-like motion. b. Life cycle and reproduction (1) All nematodes hatch from eggs as first-stage larva(L1) and metamorphose by molting through second-,third- and fourth-stage larvae (L2, L3, and L4) to become adult worms. Life cycles range from simple (e.g., ingestion of the egg is followed by development from eggs to adult in the intestine) to complex (e.g., involving tissue migration or intermediate hosts or vectors). (2) All species are diecious but some can reproduce by parthenogenesis. Intestinal Nematodes 1.Entrobius vermicularis (Pinworm) a. General properties E. vermicularis is a small, white round worm. Females average 10mm in length, males 3mm. The worm has a direct life cycle with no tissue migrate phase. b. Epidemiology (1) Distribution. E. vermicularis is a cosmopolitan, though this helminthes is most common in temperate areas. (2) Incidence and prevalence. More than 1 billion cases occur world wide. Peak prevalence is in the 5- to 6-year-old age group; 30% 40% of affected children are white, and 10% - 15% are black. Adults are more refractory, indicating that resistance may occur with age (possibly by acquired immunity). (3) Transmission. eggs deposited in a sticky secretion on the perianal skin by nocturnally wandering female worms. Eggs also contaminate bed clothes and can be aerosolized during bed making. Infection occurs via ingestion or inhalation of eggs. Entrobius vermicularis eggs, larva & adult Entrobius vermicularis life cycle Entrobius vermicularis life cycle c. Pathogenesis and clinical disease. The eggs hatch in the large intestine. Worms mature in 2-4 weeks and live for 2 months. Continuous reinfection is common. (1) approximately one-third of infections are asymptomatic. (2) The most common presentation is irritation and pruritus ani. sometimes itching is severe, and secondary bacterial infection occurs. Occasionally, necrosis of the mucosal surface produces pain when nerve endings are exposed. (3) Worms often occur in the appendix and may be associated with appendicitis, but causation has not been proved. Rarely, worms may migrate to ectopic sites, mostly within the female genitourinary tract d. Laboratory diagnosis (1) Cellophane tape test. E. vermicularis females lay their eggs on the perineum during the night. Touching the perianal skin with the sticky side of the tape will pick up the eggs; the tape is affixed to a microscope slide and examined. Eggs are oval, approximately 55X25 µm in size, and flattened on one side, and they contain a larva. (a) Specimens should be collected prior to bathing or using the toilet. (b) Four to six consecutive negative pinworm tape preparations are required to rule out infection. (2) Stool samples. Eggs are only rarely seen in stool, but in patients with heavy worm burdens, adult female worm may be seen in stool samples. e. Control and prevention Pin worm control and prevention measures include practicing proper personal hygiene, particularly hand washing; apply an ointment or salve to an infected perianal area to help prevent egg dispersal into the environment; and avoiding scratching the infected area. Furthermore, thorough cleaning of all potentially infected environment surfaces, including linens, and providing treatment to all household members are important steps to help prevent further infections. Because of the ease with which this parasite is capable of being transmitted, total eradication of pin worm is highly unlikely in the near future. Prevention of reinfection: Some physicians recommend treating the patient’s entire family. The eggs are not resistant to desiccation and usually only survive 6-12 hours, but they may remain viable for a few weeks in colder, more humid environments, bed lined and towels should be washed. Single dose of Mebendazol and Pyrantel pamoate /os (oral) are highly effective. Treatment should be repeated after 10-14 days to kill the newly acquired developing adult worms.