Lecture Notes")
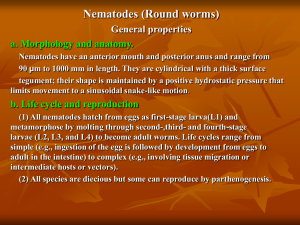
Helminths Intestinal Nematodes: Enterobius vermicularis (Pinworm):Is the most common intestinal parasitic infection worldwide. Pinworms are particularly common in children. Geographical Distribution:Pinworm is a cosmopolitan parasite with particularly high prevalence in countries with a temperate climate. Habitat: Adult worm (female resides in cecum and appendix of man). Morphology: Adult Worm: The male adult worm is 5 mm × 0.5 mm in diameter while female measures 8 to 12 mm × 0.3 to 0.5 mm. The anterior end tapers and is flanked on each side by cuticular extensions called “cephalic alae”. The esophagus is slender, terminating in a prominent posterior bulb, which is called esophageal bulb. The cephalic alae and esophageal bulb are important in identification of the species. The posterior end of female is sharp and pointed while it is curved in males. 11 Male dies after fertilization, while gravid female dies after oviposition within 2 to 3 weeks. Figure6: Adult Enterobius vermicularis (Female). Figure7: Adult Enterobius vermicularis (male). 11 Figure 8: Anterior part of Enterobius vermicularis. Egg Pinworm eggs are colorless, flattened asymmetrically on one side, ovoid, approximately 55 mm x 25 mm in size, surrounded by transparent shell and contains coiled tadpole-like larvae, and embryonate in six hours. These eggs can remain viable for about twenty days in a moist environment. Figure 9: Enterobius vermicularis egg. 11 Figure 10: Enterobius vermicularis eggs determined by Scotch-tape Technique. Life Cycle: The female worm when fully gravid passes down to migrate several inches outside the anus to deposit eggs. These eggs are transferred by fingers (autoinfection) and by contaminated food or fomites to the mouth and they are swallowed. On reaching the intestine, outer shell is dissolved by digestive enzyme thus liberating the larvae. In the presence of oxygen, larvae become infective worm. 11 Figure 11: Life cycle of Enterobius vermicularis. Pathogenicity and Clinical Picture:Pinworm infection is usually benign, and are asymptomatic. The movement of adult worm (female) at the time of laying eggs causes intense itching and the itching is usually the most severe at night. inducing the patient to scratch the affected area (anal canal 11 and perianal skin). Scratching may lead to anal lesion and perineal pruritus, which may be lead to secondary bacterial infections. Complications are generally associated with extra intestinal infections in pretoneum, kidney, liver and lungs. Heavy infections cause insomnia, nightmares, weight loss, convulsion, mucosal ulceration, submucosal abscesses, mild eosinophilic and lymphocytic infiltration and granuloma. Laboratory Diagnosis: The most common means of diagnosing pinworm infection is via the “Scotch tape” test, where a clear adhesive cellulose tape is applied to the anal area early in the morning before bathing or defecation. This is then observed under a microscope for the presence of pinworm eggs. (a minimum of four to six consecutive negative tapes is required to rule out the infection). Detection of adult worm in the stools. Demonstration of eggs in stool and finger nails, perianal skin scraping and washings from underwear. Treatment Piperazine, albendazole, and mebendazole are effective. 11