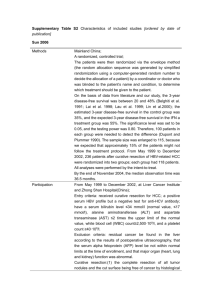
Early stage HCC management
BCLC Staging and Treatment
Schedule
HCC
Stage 0
PST 0, Child-Pugh A
Stage A-C
PST 0-2, Child-Pugh A-B
Very early stage (O)
Single < 2 cm
Carcinoma in situ
Early stage (A)
Single or 3 nodules
< 3 cm, PS 0
Portal
pressure/bilirubin
Resection
Increased
No
Liver Transplantation
(CLT/LDLT)
Curative Treatments (30%)
5-yr survival: 50-70%
ttc: treatment
Advanced stage (C)
Portal invasion,
N1, M1, PS 1-2
Terminal
stage (D)
3 modules 3 cm
Single
Normal
Intermediate stage (B)
Multinodular, Ps 0
Stage D
PST>2, Child-Pugh C
Associated
diseases
Yes
PEI/RF
Chemoembolization
Sorafenib
Randomized controlled trials (50%)
3 yr survival: 20-40%
Symptomatic ttc (20%)
1 yr survival: 10-20%
Adapted from Llovet JM et al. J Natl Cancer Inst 2008;100: 698 – 711
Levels of evidence in the assessment of benefits
in HCC treatment
Treatments assessed
Benefit
Evidence
Increased survival
Uncertain
Increased survival
Treatment response
3iiA
1iiA
3iiA
2iiDiii
Increased survival
3iiA
Better local control
Increased survival
Treatment response
Treatment response
1iiD
1iiA
3iiDiii
3iiDiii
Increased survival
No benefit
No benefit
No benefit
1iA
1iA
1iiA
1iiA
Surgical treatments
Surgical resection
Adjuvant therapies
Liver transplantation
Neoadjuvant therapies
Locoregional treatments
Percutaneous ablation
Ethanol injection
Radiofrequency ablation
Chemoembolization
Arterial chemotherapy
Internal radiation (I131, Y90)
Systemic treatments
Sorafenib
Tamoxifen
Systemic chemotherapy
Interferon
Classification of evidence adapted from the National Cancer Institute (from Llovet JM, et al. J Natl Cancer Inst 2008;100:698-711)
Level 1 = Randomized, controlled trial, meta-analysis (double-blinded, 1i; non-blinded, 1ii)
Level 2 = Non-randomized controlled trial
Level 3 = Case series (population-based, 3i; non-population-based, consecutive; 3ii; non-population-based, non-consecutive, 3iii)
Endpoints: A = Survival, B = Cause-specific mortality, C = quality of life, D = indirect surrogates (DFS, PFS, tumor response)
Llovet JM et al J Natl Cancer Inst 2008;100: 698 – 711
Surgical resection
Surgical Resection
Optimal candidates:
BCLC stage 0 or A
–
–
–
–
Child-Pugh A
Performance status 0
Single tumors (< 3 cm)
Normal portal pressure
5-year survival
60-70%
– Normal bilirubin
Excellent functional reserve
High recurrence rate
50% at 3 years
70% at 5 years
Bruix J et al. J Hepatol 2001; 35: 421-430; Llovet JM. J Gastroenterol 2005; 40: 225-235
Resection in Child A Patients offers good survival
70%
Poon RT et al. Ann Surg 2002; 235(3): 373-82.
Risk Factors Contributing to HCC Early Phase
Intrahepatic Recurrence after Hepatectomy
Factors contributing to early phase
(<2 years) recurrence
Hazard
ratio
95% CI
Microscopic vascular
invasion
2.36
1.62 – 3.45
Serum AFP value ≥ 32
ng/ml
1.83
1.25 – 2.68
Non anatomical
resection
1.65
1.13 – 2.40
Imamura H et al. J Hepatol 2003; 38: 200-207
Is resection only a palliation?
186 patients with HCC 2 cm treated with curative hepatectomy
Early HCC
Small advanced
HCC
The survival rate of patients with early HCC undergoing Liver Resection
decreases 5 years after surgery. This phenomenon is explained by
occurrence of second primary HCCs that should be prevented
Yamamoto M et al. Ann Surg. 2004; 239(3): 395-9
Liver transplantation
Liver Transplantation
Advantage
Removal of the diseased liver together with the tumor
Disadvantage
Long waiting lists
Optimal candidates:
• BCLC Stage A disease
• No vascular invasion
• No metastases
• Fulfill the Milan criteria
– Solitary tumor < 5 cm or
– ≤ 3 nodules < 3 cm
Illustration Copyright © 2007 Nucleus Medical Art,
All rights reserved. www.nucleusinc.com.
5-year survival 70%
Recurrence rate < 15%
Bruix J, Sherman M. Hepatology 2005; 42: 1208-1236; Llovet JM. J Gastroenterol 2005; 40: 225-235;
Mazzaferro V et al. N Engl J Med 1996; 334: 693-699
MILAN Criteria
• Unresectable HCC single nodule <5cm or
<3nodules <3cm
• No vascular invasion or node mets
Mazzaferro V et al. N Engl J Med. 1996; 334(11): 693-9
Liver Transplantation
Survival of patients with single HCC < 5 cm or 3 < 3 cm (n= 48)
Overall Survival %
100
75%
80
60
40
20
0
0
12
24
36
48 months
Mazzaferro V et al. N Engl J Med. 1996; 334(11): 693-9
Liver Transplantation
…The 5-year survival of liver transplantation for HCC has improved
with time (1987-2001). It is possible that the published criteria for
patient selection may have contributed to the better outcome.
Yoo HY et al. J Clin Oncol. 2003; 21(23): 4329-35
Non surgical treatments
Non Surgical Treatments:
Percutaneous Ablation
Radiofrequency ablation (RFA)
Percutaneous ethanol injection
(PEI)
Optimal candidates:
Child-Pugh A
Single tumors < 3 cm in diameter
Illustration Copyright © 2007 Nucleus Medical Art,
All rights reserved. www.nucleusinc.com.
Llovet JM. J Gastroenterol. 2005; 40(3): 225-35; Bruix J et al. Hepatology 2005; 42(5): 1208-36; Bruix J et al. J Hepatol. 2001; 35(3): 421-30
Non Surgical Treatments:
Percutaneous Ablation
Radiofrequency ablation (RFA)
Percutaneous ethanol injection (PEI)
Optimal candidates:
Child-Pugh A
PEI
5-year survival 40-50%
High recurrence rate
50% at 3 years
70% at 5 years
Single tumors < 3 cm in diameter
Llovet JM. J Gastroenterol. 2005; 40(3): 225-35; Bruix J et al. Hepatology 2005; 42(5): 1208-36; Bruix J et al. J Hepatol. 2001; 35(3): 421-30
Recurrence rates
Recurrence of HCC after curative treatment
HCC stage
Early stage (A)
1–3 nodules <3 cm,
PS 0
Very early stage (0)
Single <2 cm
carcinoma in situ
3 nodules ≤3 cm
Single
Portal pressure/bilirubin
Associated diseases
Increased
No
Normal
Potentially curative
treatment
Resection
Liver
transplantation
Yes
PEI/RFA
5-year recurrence
>70%
Possible causes
contributing to
recurrence
<15%
>70%
Proliferation of residual microscopic disease
Neovascularization
Mazzaferro V et al. N Engl J Med 1996;334:693–9; Zavaglia C et al. Am J Gastroenterol 2005;100:2708–16;
Cherqui D et al. Ann Surg 2009;250:738–46; Imamura H et al. J Hepatol 2003;38:200–07; Forner A & Bruix J. Hepatology 2008;44:5–7;
Qin LX & Tang ZY. Curr Cancer Ther Rev 2005;1:71–80; Poon R et al. J Clin Oncol 2002;20:1775–85
Magnitude of the problem:
the unmet need of prevention of recurrence
Llovet et al, 1999
100
Poon et al, 2002
Probability (%)
80
After
resection
60
40
20
0
0
12
24
32
Months
48
60
72
Months
Lencioni et al, 2005
Shiina et al, 2005
After
ablation
Llovet J et al. Hepatology 1999;29:62–7; Poon R et al. Ann Surg 2002;235:373–82;
Lencioni R et al. Radiology 2005;234:961–7; Shiina S et al. Gastroenterology 2005; 129:122–30
Patterns of HCC recurrence
Predictors of EARLY recurrence
Predictors of LATE recurrence
• Microscopic vascular invasion
• Grade of hepatitis activity
• Serum AFP value ≥32 ng/mL
• Aetiology of hepatitis
• Non-anatomical resection
• Age
Imamura H et al. J Hepatol 2003;38: 200–07;
Mazzaferro V et al. Hepatology 2006;44:1543–54; Cucchetti A et al. Ann Surg Oncol 2009;16:413–22
Haematogenous dissemination of tumour cells
after resection of HCC
Patients who developed recurrence
Patients who did not develop recurrence
AFP-expressing tumour cells are disseminated mostly post-operatively
This may potentially be the source of recurrence or metastasis
Wong GL et al. Clin Cancer Res 1999;5:4021–7
N=100
y = –0.344 + 0.24x
r2 = 0.084
P<0.001
40
30
20
10
0
80
Micrometastases in proximal area
70
Micrometastases in distal area
60
50
40
30
20
3.50
3.25
3.00
2.75
2.50
2.25
Size of main tumour (mm)
60
2.00
50
1.75
40
1.50
30
1.25
20
1.00
10
0.75
0
0
0.50
–10
0.25
10
0.00
Distance of microsatellite
(mm)
50
Number of
micrometastases (n)
Micrometastases/microsatellites could spread via
invasion of portal vein branches at an early stage
Distance of spread (cm)
Micrometastases could spread via invasion of portal vein branches
at an early stage even when the tumour is solitary and small
Sasaki A et al. Cancer 2005;103:299–306; Shi M et al. World J Surg 2004;28:376–81
Late recurrence of HCC after surgery
(Resected patients)
LOW RISK
<2 risk
factors
HIGH RISK
≥2 risk
factors
(HCC occurrence)
Risk factors for and incidence of late recurrence after surgery overlap
with those associated with HCC first occurrence in cirrhosis
Cucchetti A et al. Ann Surg Oncol 2009;16:413–22
Prognostic factors associated with risk of
recurrence
Grade of
differentation
Nuclear grade 1
Strong predictors of
HCC recurrence after
curative resection:
Microvascular invasion
• Microvascular invasion
• Grade of differentiation
• Microsatellites
Microsatellites
Nuclear grade 2
Nuclear grade 3
Lauwers GY et al (The International Cooperative Study Group on Hepatocellular Carcinoma). Am J Surg Pathol 2002;26:25–34;
Bruix J & Sherman M. Hepatology 2005;42:1208–36
Morphology: pathology correlation
The metroticket experience:
1556 HCCs studied with explant pathology
1083 pts
17%
Incidence of mVI and G3 tumours are parallel and increase
significantly with size-and-number features of HCC
Mazzaferro V et al. Lancet Oncol 2009;10:35–43
Microvascular invasion and outcome
The degree of mVI predicts outcome after resection and could be useful
to select patients for salvage transplant or to enrol patients in trials
evaluating new molecular targeted therapies
Immunoreactivity for anti-smooth muscle actin
antibody to asses presence of muscle in the wall
Roayaie S et al. Gastroenterology 2009;137:850–5
Can mVI invasion be predicted by imaging?
Wedge-shaped
peritumoural
enhancement is triangular
enhancement with the
base headed way from
the tumour
Irregular circumferential
peritumoural
enhancement: (polygonal
shape parallel
to the tumour border)
NMR findings of circumferential peritumoural enhancement showed
statistical correlation with microscopic vascular invasion
Kim H et al. Eur Radiol 2009;19:1744–51
Integrative transcriptome analysis reveals
common molecular subclasses of human HCC
• S1 tumours exhibited more vascular invasion and satellite lesion
• These results may suggest that the S1 subclass is associated with
a more invasive/disseminative phenotype
Hoshida Y et al. Cancer Res 2009;69:7385–92
Molecular markers of late recurrence
A
C
Expression
pattern of 186
gene-survivalsignature
OS according
to the level of
expression of
the 186 genes
among 168 pts
with longer
duration of
follow-up
B
D
OS according
to the level of
expression of
the 186 genes
among 225
tissue validation
samples
Probability of
late-recurrence
according to
the expression
of the laterecurrence
gene signature
A reproducible gene signature correlated with survival
in liver tissue adjacent to the tumour
Hoshida Y et al. N Engl J Med 2008 359:1995–2004
Liver regeneration pathways after resection
are partially shared by HCC cell proliferation
TGF
uPA/plasminogen
Pro-HGF
HGF
Met
Stellate cell
Hepatocyte
P13K
AKT
S6 kinase
TGF
Cyclin E
AP1
JNK
pERK
C/EBP
IGFBP1
VEGF
Endothelial cell
P27
Cyclin D
TOR?
Hepatocyte
A Growth factor-dependent
LPS
C3a
C5a
ICAM
B Cytokine-dependent
IL-6
TNF
PAI
SCF
STAT3
Hepatocyte SOCS3
Kupffer cell
A: Growth factor-dependent
B: Cytokine-dependent
• HGF activate hepatocyte regeneration through
downstream pathways (PI3K, pERK, AKT)
• IL-6 and TNFα are crucial priming stimuli
activating STAT 3, MAPK and pERK
• VEGF activate proliferation of endothelial cells
Taub R et al. Nat Rev Mol Cell Biol 2004;5:836–47
Recurrent HCC after curative treatment:
adjuvant strategies
Chemotherapy
- HCFU
- UFT
- Epirubicin + cisplatin
- Capecitabine
…..
Adjuvant immunotherapy
- Adoptive
immunotherapy
- Tumour vaccines
- Interferon
Vitamin chemoprevention
- Vitamin A
- Vitamin K
…..
Adjuvant
systemic
strategies
Novel agents
Chemotherapy
No evidence of benefit from adjuvant chemotherapy compared to surgery
alone in improving survival rates after curative tumour resection
The potential benefits of CT on tumour recurrence should be weighed against
the risk of adverse reactions in patients with an underlying liver dysfunction
Samuel M et al. Cochrane Database Syst Rev 2009;CD001199
Chemotherapy:
RCT using UFT (uracil + tegafur)
A. Recurrence-free survival
B. Overall survival
100
100
UFT
80
80
Patients (%)
Patients (%)
Control
60
40
20
60
UFT
40
Control
20
0
0
0
1
Patients at
risk
UFT
79 53
Control 80 58
2
3
4
5
6
Years
38
43
32
29
20
19
18
13
9
4
7
8
0
1
Patients at
risk
UFT
79 79
Control 80 80
2
3
4
5
6
7
35
40
19
21
7
8
8
Years
78
79
72
75
54
56
• No evidence to support potential benefit of adjuvant
UFT, an oral agent which combines uracil and 5FU
prodrug
• Such treatment may even worsen OS
Hasegawa K et al. Hepatology 2006;44:891–5
Adjuvant immunotherapy:
adoptive immunotherapy
Autologous lymphocytes activated with recombinant
interleukin-2 and antibody to CD3
Immunotherapy
Control
Recurrence-free (%)
100
80
60
40
20
P=0.008
0
0
1
2
3
4
5
6
7
Time after hepatectomy (years)
• Safe, feasible and lowers tumour recurrence
• No significant difference in OS
Takayama T et al. Lancet 2000;356:802–7
Adjuvant immunotherapy:
role of IFN
Clavien PA. Ann Surg 2007;245:843–5
IFN may prevent late recurrence after HCC resection
in specific subgroups of HCV cirrhosis
HCV pure patients
Mazzaferro V et al. Hepatology 2006;44:1543–54
Vitamin chemoprevention of recurrence:
retinoids
Oral polyprenoic acid prevents late recurrence
after surgical resection or PEI
Muto Y et al. N Engl J Med 1996;334:1561–7;
Takai K et al. Intervirology 2005;48:39–45
Recurrent HCC after curative treatment:
adjuvant strategies
Chemotherapy
Adjuvant
systemic
strategies
Adjuvant immunotherapy
Vitamin chemoprevention
- HCFU
- UFT
- Epirubicin + cisplatin
-Capecitabine
…..
- Adoptive
immunotherapy
- Tumour vaccines
- Interferon
- Vitamin A
- Vitamin K
…..
Level II clinical evidence does not support the use of systemic adjuvant
therapy, tested for resectable HCC
Based on the current evidence, there is no role for the aforementioned
adjuvant strategies therapy in the management of HCC