Powerpoint File
advertisement

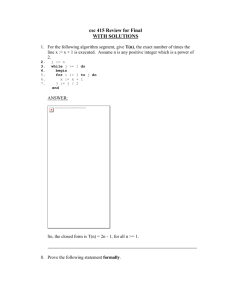
Problems with ileostomies Mr Paul S Rooney Colorectal surgeon Royal Liverpool Hospital ileostomy End (Brown 1930) Everted (Brooke 1952) Loop (Turnbull 1961) Generic Problems Eczema Poor seal Sweating Hygiene Psychological (unnecessary changing) Physical and metabolic Physical problems Retraction Ischaemia Necrosis Abscess Fistula Recurrent disease Bleeding Hernia Pyoderma Everting wrong end Tension,obesity Iatrogenic Crohns,Cancer Varicies negligence Varices Portal hypertension ALD Sclerosing cholangitis Liver mets Treatment Injection of sclerosant , phenol,alcohol. Needs repeat every 6weeks (Major 86) Muco-cutaneous disconnection easy! 20% recurrence in 30 months (Beck 88) Hernia 10-40% 20% require surgery (pain,obstruction etc) Repair by non absorbables 50% recurrence rate.(Allen-Mersh (1988) Mesh or Move? Heamatoma Infection Erosion Low recurrence rate<1%@5y (Bokey 2003) Laporotomy risk? Poorly sited likely to benefit Decision depends on patient factors and number of previous repairs ileostomy Flux Normal 3-800ml/day >10cm resection significantly increases flow Infection Radiation Crohns, cancer Obstruction 4-5l/day! Flux Losses of >1L need replacing as saline 1.5l need admitting Can fatally induce Addisonian crisis 100mg hydrocortisone qds (lifesaving) Renal failure Somatostatin PPI’s Metabolic Chronic dehydration Anaemia ,low ferritin Low B12, Na, K Urate and calcium stones Gall stones (loss of bile salts) Closure V easy or VV Hard Try to avoid early closure wait 6 weeks at least 50% complication rate inc death! No one way of closure appears to be best (Hosie 1991) Stoma problems: Retraction Excoriation Prolapse Necrosis