phlebothrombosis
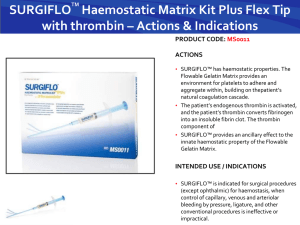
advertisement

MUDr. Monika Laššánová THROMBOSIS = INTRAVITAL COAGULATION OF BLOOD IN VESSELS OR HEART Incidence of venous thromboembolism – 0,1% – 0,01% among people appr. 20 years old – 1,0% among people appr. 60 years old Patogenesis of thrombosis = (1856) – Wirchow´s trias Most important factors activation of COAGULATION = activity of TXA2, activity of anticoagulant sys. (AT III), levels or activation of coagulation f. ... slow BLOOD FLOW = stasis, travelling by airplain, heart failure, paraplegia, immobilisation, pregnancy, varixes, operations, fractures ... deffect of the VESSEL WALL – by damage of endothelium production of PGI2 => proaggregatory activity Arterial thrombi = white – Thrombocytes – Tight adherence => obturation = periferal ischemia – Prevention = antiaggregants Venal thrombi = red – Fibrinal tail – Weak adherence => risk of embolisation – Prevention = anticoagulants Recent thrombi – Are removed by thrombolytics = fibrinolytics Clinical conditions increasing the risk of thrombosis arterial: atherosclerosis smoking hypertension diabetes mellitus LDL TAG + family history deffect of left high doses of synthetic oestrogens polyglobulia … venous: general surgery orthopedical surgery trauma, malignities, sepsis immobilisation congestive failure nephrotic syndrome obesity varixes postphlebitic syndrome oestrogens pregnancy Different! thrombophlebitis phlebothrombosis THROMBOPHLEBITIS primarily caused by mechanical, microbial or chemical irritation inflammation of vessel wall secondarily thrombosis – thrombus firmly adhering to vessel wall embolisation only occasionally clinically: local syndrome = inflammated superficial vein, can be palpated, skin above is red, warm, with significant pain and sensitivity, no big oedema, no general symptoms or only subfebrility complications: (rarely) early – spreading of inflammation to deep venous sys., late – sec. chronic venous disease = postphlebitic syndrome Deep Venous Thrombosis = Phlebothrombosis + it´s most dangerous complication = pulmonary embolisation (PE) – belong (after IHD and hypertension) among the most common CV diseases in hospitalised patients PE - 10% of autopsial material 85% of PE is caused by deep venous thrombosis PHLEBOTHROMBOSIS (PT) deep veins of lower extremities primarily obturation of vein with thrombus and secondarily inflammatory reaction released thrombus = embolus clinically: often asymptomatic – or little symptoms = dg. only 30-50% – oedema – asymmetric – pain – spontaneous, compressive – mostly while hanging down the limb, spasms, feeling of strain – symptoms of blocked blood flow from the limb (erythemapale skin- cyanosis) – collaterals –forming after several days of obturation as compensatory mechanism, – systemic symptoms – not specific (if there is no PE) Clinical symptoms Lower limb: pain oedema ( 1,5 cm) posit. palp. maneuvers (Homans, Lőwenberg,...) enlarged superficial collaterals change of skin color and temperature Complications of PT 1. EMBOLUS - released thrombus, carried by the blood flow– mainly to pulmonary artery pulmonary embolisation 2. Repeated small embolisation (successive) =>chronic pulmonary hypertension => cor pulmonale chronicum 3. Chronic venous insufficiency Diagnosis of DVT + - Kontrastná venografia - Impedančná pletysmogr. Goals of the treatment of PT save the patient´s life avoid occurance of pulmonary embolism initialise / speed-up resolution of thrombus/embolus accelerate symptom regression prevention of recurrency Prevention of PT nonpharmacologic limb elevation (15-20º) early mobilisation after surgery regular exercise with legs in bed elastic, special tights walking pharmacologic low doses of heparin (5000 IU) (before operation, during postoperation period at risk patients), LMWH, fondaparinux Antithrombotics Antiaggregatory drugs Anticoagulants Thrombolytics (inh. platelets) (inh. coagulatory factors) (dissolve thrombus) Antithrombotics antiaggregants (antiplatelet drugs) = block FORMATION of thrombus anticoagulants = block GROWTH of thrombus thrombolytics (fibrinolytics) = DISSOLUTION of already formed thrombus Equilibrium Between Coagulation and Fibrinolysis Antiplatelet drugs Anticoagulants Thrombolytics Anticoagulants DRUGS ARTIFICIALLY INDUCING “DISTURBANCES“ OF BLOOD COAGULATION GOAL: TO PREVENT THROMBOSIS OR TO PREVENT FURTHER GROWTH OF THROMBUS Coagulation Cascade ANTICOAGULANTS DIRECT Indirect inhibitors of thrombin and factor Xa – Heparin (IIa : Xa) – LMWH (IIa : Xa) enoxa-, fraxi-, dalte-, revi- – Fondaparinux ( Xa) Direct inhibitors of thrombin – Hirudin, bivalirudin, desirudin – Dabigatran – p.o. = gatrans Direct inhibitors of factor Xa Rivaroxaban – p.o. = xaban Apixaban – p.o. INDIRECT Warfarin Etylbiskumacetate Phenprocoumon Dicumarol Fondaparin Idraparin indirect anticoag. f. II., VII., IX., X Rivaroxaban Apixaban Dabigatran Hirudin, Desirudin indirect inhibitors of thrombin HEPARIN INDIRECT INHIBITOR OF THROMBIN SUBSTANCE PRESENT ALSO IN OUR BODY (MAST CELLS), USED FROM 1916 MW = 3 - 30 000 D (15 000 D) produced from intestinal mucosa of porcine or cattle lungs => quantified in IU heterogenous mucopolysacharid, anion (´-´ charge) ACTIVITY IS DEPENDENT FROM THE PRESENCE OF A N T I T H R O M B I N III. Mechanism of Action of Heparin - + 1000x H inactivates already activovated coagulation factors IIa, Xa Effects of heparin Anticoagulatory activity Weak inhibition of platelet function - adhesivity and aggregation Weak stimulation of fibrinolysis releasing of lipoproteinic lipase clearing of lipemic plasma anti - IIa : anti –Xa = 1 : 1 Advantages of heparin acts very quickly or immediately, but shortly has massive effect it has an antidote - protamine Disadvantages of heparin only injection (i.v., s.c.), i.m. – no, irregular absorption and haematoma T1/2 is variable, prolonged with dose, unpredictable anticoagulant effect – wide variability (for different binding to proteins and unpredictable absorption after s.c. admin.) possibility of disease reactivation after stopping administration (rebound efect) control: aPTT (reflects effect to thrombin) – extension to 1,5-2,5 x of norm aPTT = 1,5-2,5 x normal Indications of heparin Prophylaxis of vein thrombosis Th. of deep vein thrombosis and pulmonary embolia Acute coronary syndroms (Th) Obturation of peripheral arteries Hemodialysis, DIC ADR of heparin Bleeding H. induced thrombocythopenia (HIT) – less serious, early f.; more serious f. after 5 and days Allergy Reversible alopecia Possible osteoporosis in case of longterm use LOW-MOLECULARWEIGHT HEPARINS (LMWH) INDIRECT INHIBITORS OF THROMBIN smaller molecules, MR 5 000 D INHIBIT MORE ANTI-Xa PRODUCED BY CHEMIC OR ENZYMATIC DEPOLARISATION OF H ACTIVITY DEPENDS ON THE PRESENCE OF A N T I T H R O M B I N III Mechanism of LMWH Action anti - IIa : anti -Xa 1 : 2-4 Indications of LMWH Prevention of thromboembolia (abdominal and orthopedic surgery) Prevention of ischemic complications at acute coronary syndroms (unstable angina pectoris, NSTEMI myocardial infarction) Therapy of phlebothrombosis and pulmonary embolism Hemodialysis Advantages of LMWH Predictable response to dose according to weight Longer plasmatic half-life (1-2 s.c. injections per day) Lower risk of thrombocytopenia, bleeding and thrombosis Heparin and LMWH can be administered during pregnancy and lactation Fondaparin Idraparin indirect anticoag. f. II., VII., IX., X Rivaroxaban Apixaban Dabigatran Hirudin, Desirudin direct inhibitors of thrombin FONDAPARINUX INDIRECT INHIBITOR OF THROMBIN SYNTHETIC PENTASACHARID SPECIFICALLY INHIBITING FACTOR Xa MR = 1 700 D activity depends on the presence of I T H R O M B I N III ANT doesn´t have the long chain needed for bridging to ATIII. and f. IIa 300X ability to inactivate f. Xa MA of Fondaparinux Advantages of Fondaparinux of bleeding complications administered s.c. relatively long lasting effect highly predictable effect doesn´t influence aggregation of platelets doesn´t induce thrombocythopenia disadvantage = price, no antidote Fondaparin Idraparin Indirect anticoag. f. II., VII., IX., X Rivaroxaban Apixaban Dabigatran Hirudin, Desirudin direct inhibitors of thrombin HIRUDIN, BIVALIRUDIN PRIAMY INHIBÍTOR TROMBÍNU špecificky IREVERZIBILNE INAKTIVUJE TROMBÍN BEZ potreby prítomnosti AT III. je prirodzený inhibítor zrážania krvi získavaný z pijavíc (hirudo medicinalis) vyrába sa DNA REKOMBINANTNOU technikou HIRUDIN, BIVALIRUDIN DIRECT INHIBITOR OF THROMBIN SPECIFICALLY IRREVERSIBLY INACTIVATES THROMBIN WITHOUT THE NEED FOR AT III NATURAL INHIBITOR OF BLOOD COAGULATION GAINED FROM LEECH (HIRUDO MEDICINALIS) PRODUCED BY DNA RECOMBINANT TECHNOLOGY MA HIRUDIN BINDS TO THROMBIN AND irreversibly FORMS AN INACTIVE COMPLEX BIVALIRUDIN - synthetic fragment of hirudin - reversible inhibition of thrombin - duration of action appr. 25 min. Advantages of Hirudin doesn´t bind to plasma proteins predictable anticoagulant effect indicated for patients with thrombocythopenia after heparin who need AC th. bivalirudin – indicated in AMI, as an alternative to heparin/LMWH inactivates not binded thrombin, but also thrombin binded to fibrin in thrombus anticoagulatory effectivity inhibits formation of fibrin inhibits activation of thrombocytes = mild antiaggregatory effect prevents activation of f. V, VIII, XI and XIII peg-hirudin – 1 times per day, s.c. Newer peroral anticoagulants Dabigatran- direct inhibitor of thrombin; approved for prevention of thrombosis after hip or knee surgery; atrial fibrillation (prevention of thr.) Rivaroxaban- direct inhibitor of factor Xa; approved for prevention of thrombosis after hip or knee surgery; atrial fibrillation (prevention of thr.) DABIGATRAN (g a t r a n s) Potent, competitive, direct, reversible inhibitor of thrombin Ximelagatran hepatotoxicity Inhibits: – Free thrombin – Thrombin binded to fibrin – Tr. aggregation induced by thrombin Potent, predictable anticoag. effect !!! p.o., rapid onset + long duration Few interactions with drugs and food No need for regular coagulation controlls I: primary prevention of thromboembolic dis. !!! No antidote, high price !!! Fondaparin Idraparin Indirect anticoag. f. II., VII., IX., X Rivaroxaban Apixaban Dabigatran Hirudin, Desirudin direct inhibitors of thrombin RIVAROXABAN, APIXABAN (x a b a n s) Direct inhibitors of f. Xa Selective, competitive, potent Inhibits f. Xa – free, - bound with prothrombin, - also in fibrin clot (5x) Anticoag.effect is directly proportional to the level in plasma and last only during this time!! !!! p.o., fast onset of action No complicated metabolism => drug Fondaparin Idraparin indirect anticoag. f. II., VII., IX., X Rivaroxaban Apixaban Dabigatran Hirudin, Desirudin direct inhibitors of thrombin COUMARINS INDIRECT p.o. ANTICOAGULANTS = „ANTAGONISTS“ OF VITAMIN K factors II., VII., IX., X. DOESN´T ACT ANTICOAGULATORY IN VITRO Warfarin – the most widely used coumarin Other use – poison for gnawers Mech. of Action Warfarin inhibition of epoxidreductase, decreased formation of active form of vitamin K no activation of -carboxylase and no carboxylation of -glutamin residuums of factors II., VII., IX., X. + inhibition of protein C and S carboxylation coumarins antagonise liver synthesis of f. II, VII, IX and X => formed molecules are incomplete, unfunctional, can´t get activated and don´t participate in coagulation Pharmacokinetics of warfarin EFFECT STARTS WITH LATENCY OF 1224 HOURS, MAXIMAL EFFECT AFTER 2-3 days AFTER discontinuation the effect REMAINS 4-5 days 100% BA, 97% binding to plasma proteins many interactions Interactions of Warfarin pharmacokinetic - high binding to plasma proteins - metabolised by CYP 450 pharmacodynamic - groceries with high vitamin K content can reduce effect - antibiotics that suppress bacteria in GIT that produce vitamin K can increase the effect Amount of vit. K in selected groceries/food (v μg/100 g) calabresse celery cabbage dill cole chive parsley 270 300 817 400 300 380 700 spinach 500 sauerkraut 1540 oliv. oil 400 soja oil 542 sunflow. oil 10 green tea 712 chicken 300 DISADVANTAGES of warfarin latency of effect (2-3days) not suitable for therapy of a c u t e conditions => used for prophylaxis Need for control of therapy and correct dosage according to INR (2,0-4,5 – according to indication) Testing of INR every 3-4 weeks INR International normalised ratio patient´s Quick time INR = Quick time of standard Prophylaxis of thrombosis INR = 2,0 – 2,5 Therapy of thrombosis INR = 2,0 – 3,0 In pat. with antiphospholipid sy. INR = 3,0 – 4,5 Selfmonitoring INR INDICATIONS Most commonly longterm –> after previous heparinisation Prevention of venous (and sometimes arterial) thrombosis (AF, dilatative CMP, artificial valves, after deep v. thr. and pulmonary embolia,...) Advantage: 1times per day per os => also at home KI conditions with possible bleeding pregnancy – teratogen! low compliance of the p. ADR of coumarins Bleeding Teratogen Bleeding at new born whose mother takes warfarin and brest-feeds Dyspepsia Skin necrosis Treatment of warfarin induced bleeding - at mild bleeding – lower the dose or stop administration - at more severe bleeding – vitamin K - at massive bleeding – frozen plasma, prothrombin concentrate, full blood Coumarin skin necrosis IDEAL ANTITHROMBOTIC: p.o. (also parenteral at acute situations) fast onset of action high efficacy withoutDoes need of not monitoring exist low interindividual variability low interaction potential has an antidote good pharmacoeconomy Equilibrium Between Coagulation and Fibrinolysis Schematic Illustration of Fibrinolysis Abbreviations: tPA – tissue plasminogen activator; PAI – plasminogen activator inhibitor; PLG - plasminogen; AP antiplasmin; FDPs – fibrin(ogen) degradation products. Scheme and the position of the fibrinolysis activators or inhibitors FIBRINOLYTICS = thrombolytics cause/accelerate thrombus dissolution by degradation of fibrin have strict indications and contraindications, because they risk of bleeding 4x treatment must be combined with anticoagulant and/or antiaggregatory th. control: thrombin time – 2-3x extended indications: myocardial infarction, massive pulmonary embolism, DVT 1st generation: – Streptokinase – Urokinase – Anistreplase: plasminogen-streptokinase activator complex (APSAC) 2nd generation: – Alteplase (tPA, tissue plasminogen activator) 3rd generation: – Reteplase (rPA, recombinant. plasm. activator) – Lanoteplase (nPA) – Tenecteplase(TNK, recombinant. plasm. activator) – Staphylokinase Classification according to Fibrin Specificity not fibrin specific not selective Streptokinase Antistreptase Urokinase fibrin specific selective Activation of plasmin is systemic, are degraded also other proteins => ADRs Alteplase Reteplase Lanoteplase Tenecteplase Activate plasmin on the top of fibrin and less in circulation => lower risk of systemic bleeding Indications AMI (STEMI) massive pulmonary embolia acute obturation of an artery deep vein thrombosis (not always) acute thrombotic stroke In patients with ischaemic stroke we need to apply thrombolysis till 3 hours after beginning of ischaemia. At pulmonary embolia, the time interval is much longer – even several days after beginning, but the risk of bleeding to pulmonary parenchyma is higher then. ADRs frequently - bleeding including bleeding to CNS (appr. 3-4 cases /1000 treated patients) febrile reactions hypotension allergic reaction after streptokinase or anistreplase, even anaphylactic shock Absolute Contraindications stroke in last 6 months, history of bleeding to the brain serious trauma or operation in the last 3 weeks bleeding to GIT dissected aneurysm of aorta known bleeding defect I. GENERATION: NONFIBRIN-SELECTIVE AGENTS STREPTOKINASE INDIRECT activator of fibrinolytic system the oldest fibrinolytic /1933/, low price Mechanism of Action of Streptokinase 1:1 DISADVANTAGES of STK activates also the circulating plasminogen from -haemolytic streptococcus antigenic is possible to premedicate- i.v. hydrocortisone before administration of STK can cause febrile reaction effect can be reduced by streptococcal infection or previous thrombolysis with STK it can be risky to administer repeatedly – possible occurence of allergic reaction doesn´t have to be effective, will react with already formed circulating antibodies don´t administer from 5th day till 12th month after previous aplication II. GENERATION: THROMBOLYTICS FIBRIN-SELECTIVE ALTEPLASE DIRECT activator of fibrinolytic system high selectivity for plasminogen on the top of thrombus (on the top of thrombus activates plasminogen 100x stronger than in circulation) natural protease from endothelium of vessels (tPA) produced by recombinant technology short T1/2 => in continual infusion not antigenic => Ø allergies, possibility of repeated administration III. GENERATION: THROMBOLYTICS FIBRINSELECTIVE - better pharmacokinetics - fibrinolytic effect - smaller resistency to natural inhibitors - fibrin specificity with better safety profile RETEPLASE Single-chain mutant of natural tPA Produced by cultures of E. coli Not antigenic Extended T1/2 => in 2 bolus doses à 30 min. => possibility of pre-admission treatment of AMI Preferably activates plasminogen binded to fibrin => increased fibrinolytic activity TENECTEPLASE 3-multiple mutant of tPA => Even longer T1/2 than reteplase + fibrin selectivity As one i.v. bolus during 5-10 sec. Acute ST-Elevation Myocardial Infarction (STEMI) Percentage of successful vessel recanalisation (A) and mortality in 30 days (B) in clinical studies of thrombolytic therapy of acute myocardial infarction. Guideline of Therapy of DVT - 1 Heparin – Bolus: 80 IU/kg – Infusion: 18 IU/kg reached faster therapeutic values of aPTT as at - Nowadays prevention of thromboembolic disease fixedfor scheme fondaparinux be -given aPTT =can 1,5also - 2,5 3,0 x of normal values - 1 x per day s.c. aPTT every 6 hours and dose adjustment - No need for monitoring control of blood count: 3. - 5. day LMWH – adequate replacement – same effect, 1 – 2 x daily, s.c. – nowadays PREFERABLY used!!! Guideline of Therapy of DVT - 2 After reaching effective anticoagulation with heparin, long-term p.o. warfarinisation is started giving warfarin on 1st day (5mg) ~ INR ending heparin on 5th day of warfarinisation Goal: INR 2,0 - 3,0 Lenght of warfarinisation is questionable – at least 3 months after the first episode of thrombosis