J Clin Oncol
advertisement

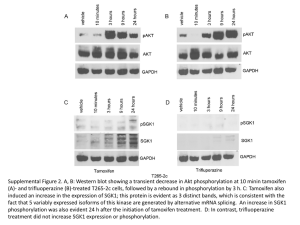
Clinical Updates Hormonally Sensitive, Early-Stage Breast Cancer Hormonally Sensitive Early-Stage Breast Cancer Current Considerations and New Directions Terry Mamounas, MD, MPH Professor of Surgery Northeastern Ohio Universities College of Medicine Medical Director Aultman Cancer Center Canton, OH Breast Cancer Mortality in US and UK WHO Mortality and UN Population Estimates Factors Associated with Reduction In Breast Cancer Mortality Early Detection Mammography LR Therapy Surgery XRT Treatment of Advanced Disease Hormonal Therapy, Chemotherapy, Trastuzumab Adjuvant Systemic Therapy Hormonal Therapy and Chemotherapy Overview Analysis: Benefit from Tamoxifen 2005 Overview Analysis Current Considerations and New Directions with Endocrine Therapy • Recurrence patterns of ER-positive BC • Optimal tamoxifen duration • Aromatase Inhibitors – Overview of efficacy data – Remaining questions • Combinations of AIs with other promising agents: – EGFR Inhibitors – mTOR Inhibitors – Bisphosphonates Long-Term Risk of Breast Cancer Recurrence Remains High in ER+ Patients 0.3 Recurrence hazard rate ER+ (n=2,257) ER– (n=1,305) 0.2 0.1 0 0 1 2 3 4 5 6 7 8 9 10 11 12 Years • A substantial proportion of breast cancer recurrences occur >5 years postsurgery • The annual risk of late recurrence is higher in ER+ tumors Saphner et al. J Clin Oncol. 1996;14:2738. More Than Half of Breast Cancer Recurrences and Deaths Occur Post-Tamoxifen Recurrences 15% 100 17% 9% 100 85.2 55% 62.7 54.9 40 Tamoxifen Control % of patients 68% 73.7 20 91.4 80 68.2 60 18% 80.9 76.1 80 % of patients Breast Cancer Deaths 87.8 73.0 73% 73.2 64% 60 64.0 40 Tamoxifen Control 20 0 0 0 5 10 Years 15 0 5 10 15 Years Adapted with permission. Early Breast Cancer Trialists’ Collaborative Group Meeting, 2000. NSABP B-14 Tamoxifen Duration Disease-Free Survival Node-Negative ER-Positive 100 Randomization Registration 80 Placebo X 5 yrs TAM X 5 yrs Placebo X 5 yrs TAM X 5 yrs TAM X 5 yrs 60 TRT PLAC TAM 40 0 1 2 N 569 583 Events 106 137 3 4 5 p=0.03 6 7 Years Fisher et al: JNCI, 2001 Adjuvant Tamoxifen Postmenopausal women with invasive tumors Preliminary Data RANDOMIZE Longer Against Shorter (ATLAS) Tamoxifen 20 mg PO qd × 5 years Tamoxifen 20 mg PO qd × 10 years N = 11,500 Woman Years Number of Recurrences Annual Rate of Recurrence Years 5 - 9 42,000 1353 3% Years 10 - 14 8000 211 3% Recurrence 3.4% × 5-yr tamoxifen Annual Event Rate 2.9% × 10-yr tamoxifen Breast Cancer Mortality Annual Event Rate 1.5% × 5-yr tamoxifen 1.4% × 10-yr tamoxifen Rate Ratio 0.866 SE (0.048) Rate Ratio 0.895 SE (0.070) Peto R, et al. 30th Annual San Antonio Breast Cancer Symposium. December 13-16, 2007; San Antonio, TX. Abstract 48. ATLAS Preliminary Results • Partial data suggest – About 12% risk reduction in breast cancer recurrence years 5 - 9 from diagnosis with continued tamoxifen • Limitations – Incomplete biomarker testing – 59% confirmed ER(+) – Adherence ~ 80% – Incomplete toxicity profile Peto R, et al. 30th Annual San Antonio Breast Cancer Symposium. December 13-16, 2007; San Antonio, TX. Abstract 48. Adjuvant Tamoxifen To Offer More Postmenopausal women with invasive tumors who received ≥ 2 years of tamoxifen N = 6934 RANDOMIZE (aTTom) Discontinue Tamoxifen 20 mg PO qd Tamoxifen 20 mg PO qd × 5 additional years Median Follow-up 4.2 Years of 15-Year Analysis Preliminary Data N = 6952 Discontinued Tamoxifen Continued Tamoxifen Relative Risk P Value Disease Recurrence 447 445 0.95 NS Gray R, et al. J Clin Oncol. 2008;26(15S): Abstract 513. Primary Endpoint: Disease Recurrence 40 No. Patients % Recurred 35 No. Obs. Events Exp. Continue 3468 437 447-9 Stop 3484 456 445-1 35% 34% 30 25 20 RR = 0.95 (0.83 - 1.09; P = NS) 15 10 continue stop 5 0 0 1 2 3 4 5 6 7 8 9 10 11 12 Years From Randomization At risk: continue 3468 3152 2831 2320 1803 1303 916 629 422 254 139 54 8 stop 3484 3160 2829 2308 1786 1284 916 635 412 250 122 49 11 Gray R, et al. J Clin Oncol. 2008;26(15S): Abstract 513. Preliminary aTTom Results • Limitations – Confirmed ER(+) = 40% – Various durations of tamoxifen use – Adherence ~ 80% – Incomplete toxicity profile • Statistically, only 68% of the true effect of 10-year tamoxifen will be observed Gray R, et al. J Clin Oncol. 2008;26(15S): Abstract 513. Adjuvant Aromatase Inhibitors Replacing 5 Years of Tamoxifen as the Gold Standard Three Strategies AIs as Initial Therapy AIs After 2-3 Yrs of TAM TAM X 5 Yrs TAM X 5 Yrs AIs After 5 Years of TAM AI X 5 Yrs TAM X 5 Yrs AI X 5 Yrs TAM X 2-3 AI X 2-3 PLAC X 5 Yrs Relative Reductions in DFS Event in 8 Reported AI Adjuvant Trials 70 60 Anastrozole Letrozole Exemestane ITA 52 m Percent 58% 50 40 IES 55 m 30 20 10 ATAC 68 m BIG 26 m ABCSG/ ARNO 28 m MA.17 30 m 40% 42% ABCSG-6 60 m 36% B-33 30 m 32% 24% 19% 13% 0 Up-Front Howell A, et al: SABCS 2004 Thurlimann et al. N Engl J Med 2005. After 2-3 yrs of TAM Coombs et al. ASCO 2006 Boccardo et al. ASCO 2005 Jakesz et al. Lancet 2005. After 5 yrs of TAM Goss et al. JNCI 2005 Jakesz et al. ASCO 2005 Mamounas et al. SABCS 2006 Reductions in Contralateral BC in 7 Reported AI Adjuvant Trials 70 Anastrozole Letrozole Exemestane 75% Percent 60 50 40 ATAC BIG 1-98 68 m 26 m 42% 30 B-33 30 m 42% (ns) ITA 36 m IES 37 m 50% (ns) 50% MA.17 30 m ABCSG/ ARNO 28 m 46% 25% 20 10 0 Up-front Howell et al. SABCS 2004. Thurlimann et al. ASCO 2005. After 2-3 y of TAM Boccardo et al. JCO 2004 Coombs et al. SABCS. 2004. After 5 y of TAM Jakesz et al. SABCS 2004. Goss et al. JNCI 2005. Mamounas et al. SABCS 2006 Aromatase Inhibitors Remaining Questions • Are there significant differences in efficacy and toxicity between different AIs? • What is the proper time to initiate AIs? • What is the optimal duration of AIs? • What is the role of AIs in premenopausal women who undergo ovarian function suppression? • What is the role of AIs in patients with DCIS NCIC MA.27 Trial: Anastrozole vs. Exemestane Placebo 3 years Anastrozole 5 years Postmenopausal ER+ and/or PgR+ Chemo or not Exemestane 5 years Celecoxib 3 years Placebo 3 years Celecoxib 3 years Activated: 6/03 Accrual: 6,830 NCIC MA.27 Trial: Anastrozole vs. Exemestane Placebo 3 years Anastrozole 5 years Postmenopausal ER+ and/or PgR+ Chemo or not Exemestane 5 years Activated: 6/03 Accrual: 6,830 Celecoxib 3 years Placebo 3 years Celecoxib 3 years Head-to-Head Adjuvant Phase IIIb Trial: Femara® vs Anastrozole Clinical Evaluation (FACE) Early Breast Cancer • Postmenopausal • ER+ and/or PgR+ • Node-positive • Primary end point: R A N D O M I Z E Letrozole 2.5 mg/d N=4,000 Anastrozole 1 mg/d Disease-free survival • Secondary end points: Safety, overall survival, time to distant mets, time to CBC, BC-specific survival De Boer et al. J Clin Oncol. 2006;24(18S):582s. BIG 1-98 Trial Design Tamoxifen 20 mg n=2,446 Letrozole 2.5 mg n=2,446 RANDOMIZATION (Following complete tumor resection) 0 Tamoxifen 20 mg Letrozole n=1,530 Letrozole 2.5 mg Tamoxifen n=1,530 2 5 years Sequential Treatment Comparisons Median Follow-up 71 months Tam→Let vs. Let Let→Tam vs. Let Mouridsen HT, et al: SABCS 2008, Abstr. 13 Breast Cancer Events TamLet vs. Let Overall By Nodal Status* *42% of the population is node positive; 58% node negative Mouridsen HT, et al: SABCS 2008, Abstr. 13 Breast Cancer Events LetTam vs. Let Overall By Nodal Status* *42% of the population is node positive; 58% node negative Mouridsen HT, et al: SABCS 2008, Abstr. 13 TEAM Exemestane vs. Tamoxifen Tamoxifen 5 y TEAM Exemestane 5 y Completed accrual: 5,700 pts (1,600 pts from US) TEAM Trial Amendment: TAM 2-3 y EXE 2-3 y TEAM EXE 5 y MA.17: Disease-Free Survival Hazard Ratios of Letrozole to Placebo 0.8 Upper 95% CL Hazard ratio 0.6 Ratio estimate 0.4 Lower 95% CL 0.2 P<0.0001 for hazard ratio trends based on time dependent Cox model 0.0 0 6 12 18 24 30 36 42 48 Months after randomization Ingle JN, et al: San Antonio, 2005 # 17 Duration of AIs MA.17 Extended Adjuvant: 5 vs. 10 Yrs Tamoxifen Letrozole Placebo (n=900) (n=900) MA.17 0y 5y MA.17 Extension 10 y 15 y Status of Trial 949 patients enrolled as of August 26, 2008 Adapted from Goss. ASCO, 2004. NSABP B-42 Trial Evaluating Adjuvant AI Duration Postmenopausal, Disease-free, Stage I, II, or III invasive BC at diagnosis ER-positive and/or PgR-positive AI X 5 yrs TAM X 2-3 yrs AI X 3-2 yrs • Primary Endpoint Disease-free survival • Secondary Endpoints Overall survival Time to treatment failure Osteoporosis-related fractures Letrozole X 5 yrs Placebo X 5 yrs Current Accrual: 1,882 / 3,840 SOFT (IBCSG 24-02, BIG 2-02) Patients who remain premenopausal within 6 months after CT or receive tamoxifen alone as adequate treatment Premenopausal ER+ 10% and/or PgR+ 10% Patients with estradiol (E2) in the premenopausal range either after CT or without CT * Strata Any CT No CT R A N D O M I Z E TAM 5 y OFS + TAM 5 y OFS + EXE 5 y Target sample size: 3,000 patients *Randomization within a 6-month evaluation period after end of CT, or within 12 weeks after definitive surgery for patients with no CT. OFS = ovarian function suppression. NSABP B-35 Postmenopausal women ER- or PgR-positive DCIS Lumpectomy with free margins Randomization 1/03-6/06 Accrual: 3,104 XRT Tamoxifen Anastrozole Recent data with AIs in combination with other agents: EGFR Inhibitors mTOR Inhibitors Bisphosphonates EGFR Interaction with the ER E2 H B E R H B MMPs MAPK c-Src E2 P CoA ER ER AF1 P E2 EREs nucleus E2 Growth and survival Gefitinib in Breast Cancer Previous clinical trials in breast cancer studies showed mainly negative results1-3 Osborne et al 4 recently reported the first randomized, placebo controlled phase II study of tamoxifen and gefitinib: A modest improved PFS in patients with hormonal-naïve disease or who had completed adjuvant tamoxifen >1 year (10.9 vs. 8.8 months, P=0.31) 1Albain KS, et al SABC 2002 2Dennison SK, et al Breast Cancer Res Treat 2007 3Smith IE, et al J Clin Oncol ,2007 4Osborne CK, SABC 2007 Anastrozole +/- Gefitinib Randomized Phase II Trial Patients • Postmenopausal women • Age ≥ 18 years • Newly diagnosed ER and / or PgR positive metastatic breast cancer Gefitinib 250 mg / day + Anastrozole 1 mg / day Primary • Progression-free survival 1:1 randomization • No prior hormonal therapy, or development of metastatic disease during / after adjuvant tamoxifen Response variables Placebo + Anastrozole 1 mg / day Secondary • Objective response rate • Clinical benefit rate • Overall survival • Safety and tolerability • Measurable or nonmeasurable disease (via RECIST) • Trial closed early due to poor accrual • 94 patients randomized Cristofanilli et al, ASCO 2008, Abstract 1012 Progression-Free Survival Gefitinib + Placebo + anastrozole anastrozole (n = 43) (n = 50) Probability 1.0 of PFS Events 22 Median PFS (months)14.5 0.8 32 8.2 0.6 0.4 0.2 HR (95% CI) = 0.55 (0.32, 0.94) 0.0 0 3 6 9 12 15 18 21 24 27 50 43 35 40 23 28 13 22 9 13 6 10 5 6 3 3 1 2 1 30 Months At risk: Placebo Gefitinib Cristofanilli et al, ASCO 2008, Abstract 1012 Objective Response and Clinical Benefit Rate (RECIST) Gefitinib + anastrozole (n = 43) Placebo + anastrozole (n = 50) 60 Response rate (%) 48.8% 50 40 34% 30 20 12% 10 0 2.3% Objective response rate (CR+PR) Clinical benefit rate (CBR) (CR+PR+SD > 24 weeks) ORR, objective response rate; CBR, clinical benefit rate; CR, complete response; PR, partial response; SD, stable disease Cristofanilli et al, ASCO 2008, Abstract 1012 Neoadjuvant Letrozole +/- RAD001 (Everolimus) • Study design – Phase II, randomized double-blind placebo-controlled trial – Postmenopausal women with >T2 tumors S C R E E N R A N D O M I Z E Tumor biopsies (pretreatment) n = 138 Letrozole 2.5 mg/d Everolimus 10 mg/d Surgery Letrozole 2.5 mg/d Placebo n = 132 16 weeks Tumor biopsies (day 15) Tumor samples (surgery) Baselga et al, ASCO 2008, Abstract 530 Neoadjuvant Letrozole +/- RAD001 (Everolimus) • Higher response with combination – PE: 68.1% vs. 59.1%, P = 0.062 – US: 58% vs 47%, P = 0.035 • Greater decrease in Ki67 • Increased toxicity – Hyperglycemia, stomatitis, infections, interstitial lung disease ABCSG-12 Trial Design • • • • • • • Accrual 1999-2006 1,803 premenopausal breast cancer patients Endocrine-responsive (ER and/or PR positive) Stage I & II, <10 positive nodes No chemotherapy except neoadjuvant Treatment duration: 3 years Primary endpoint: DFS Surgery (+RT) Goserelin 3.6 mg q28d Randomize 1:1 : 1:1 Tamoxifen 20 mg/d Tamoxifen 20 mg/d + Zoledronic acid 4 mg q6m Anastrozole 1 mg/d Median follow-up: 60 months Anastrozole 1 mg/d + Zoledronic acid 4 mg q6m Gnant et al, ASCO 2008, LBA 4 ABCSG-12: Patient Characteristics Tamoxifen n = 452 Tamoxifen + ZA n = 449 Anastrozole n = 450 Anastrozole + ZA n = 449 Median Age (years) 45.5 45.3 45.8 44.5 T1 75% 75% 77% 76% ≥ T2 22% 22% 21% 22% Node Negative 67% 66% 67% 67% Grade 3 Disease 21% 20% 22% 22% Neoadjuvant Chemotherapy 5% 5% 5% 6% Breast Conservation 80% 80% 80% 80% Gnant MF, et al. J Clin Oncol. 2008;26(18S):LBA4. First Efficacy Results Median Follow-up 60 Months N = 1801 Hazard Ratio P Value Primary Endpoint: Disease-free Survival Tamoxifen vs Anastrozole 1.01 (0.79 - 1.54) .59 Endocrine Therapy + ZA vs Endocrine Therapy Alone 0.64 (0.46 - 0.91) .01 Secondary Endpoints Relapse-free Survival Endocrine Therapy + ZA vs Endocrine Therapy Alone 0.65 (0.46 - 0.92) .015 0.60 (0.32 - 1.11) .10 Overall Survival Endocrine Therapy + ZA vs Endocrine Therapy Alone Gnant MF, et al. J Clin Oncol. 2008;26(18S):LBA4. ABCSG-12: Primary Endpoint: DFS Anastrozole vs. Tamoxifen 100 90 Disease-free Survival 80 70 60 50 40 30 20 10 0 ANA TAM 0 No. of events Hazard ratio (95% CI) vs TAM 72/903 65/900 1.008 (0.79 - 1.54) P Value .593 12 24 36 48 Time Since Randomization (months) 60 72 84 Number at risk TAM 944 849 736 589 439 264 141 60 ANA 963 849 743 558 436 271 151 59 Gnant MF, et al. J Clin Oncol. 2008;26(18S):LBA4. ABCSG-12: Primary Endpoint: DFS +/- Zoledronic Acid 100 Disease-free Survival 90 80 70 60 50 40 30 Hazard ratio (95% CI) P Value vs No ZA .011 0.64 (0.46 - 0.91) 54/904 83/899 No. of events 20 ZA No ZA 10 0 0 12 24 36 48 60 72 84 838 735 565 441 265 161 60 851 744 573 434 270 131 59 Number at risk No ZA ZA 904 899 Gnant MF, et al. J Clin Oncol. 2008;26(18S):LBA4. ABCSG-12 ITT Population First Events 45 40 Number First Event 35 Locoregional recurrence 41 30 Distant recurrence 25 29 Contralateral BCA 20 15 Seconary malignancy 20 10 5 Death without recurrence 10 10 2 10 6 9 0 0 No ZA ZA Gnant MF, et al. J Clin Oncol. 2008;26(18S):LBA4. ABCSG-12 Clinical Impact • Select, premenopausal patient population – Unknown if results can be extrapolated to postmenopausal women or more advanced disease • Await data from ongoing clinical trials to confirm and expand findings – AZURE, NSABP B-34, Z-FAST/ZO-FAST, SWOG 0307 – SOFT and TEXT • Not yet practice changing Clinical Updates Hormonally Sensitive, Early-Stage Breast Cancer Hormonally Sensitive Early-Stage Breast Cancer Current Considerations and New Directions Concluding Remarks