WELCOME TO THE PICU
advertisement

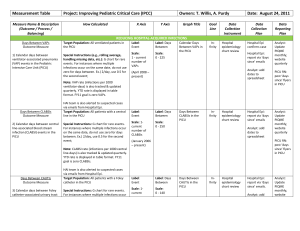
WELCOME TO THE PICU Flow Of The Day Before 8am: 8:00 - 8:30am: 8:30 - 9:00am: 9:00 - 9:30am: 9:30 - 11:00 am: 11:00 - 12:00pm: Pre-round Morning Report/ PICU Fellow Lecture (Mo/Th) Rounds (Except Fridays 9 am) Radiology Rounds Finish Rounds Work time/Didactics/First post-op admit Flow Of The Day 12:00 - 1:00pm: Noon Conference 1:00 - 4:30pm: Follow-up consultations/procedures/postop admissions/didactics 4:30 - 5:30pm: Sign-out Rounds with night team Resident Teaching Conferences PICU resident lectures: • Monday / Thursday • 8 – 8:30am • In place of morning report • At front desk in PICU Other Teaching Conferences Tuesday 12-1 PICU Fellows Conference 2E PICU Conference Thursday 12-1 PICU Conference: M&M, Journal Club, Fellows research 2E PICU Conference Educational Resources • PICU resident handbook with relevant PICU topics is available at http://peds.stanford.edu/Rotations/picu/picu_re c_readings.html Hard copy is available in the resident call room. PICU chapters at http://peds.stanford.edu/Rotations/picu/picu_rec_readings.html • • • • • • • • Monitors in ICU Vascular Access Codes ICP management Status Epilepticus Sedation Pediatric Airway Airway Management • Mechanical Ventilation • ARDS • Status Asthmaticus • Inotropes • Shock • Sepsis • Meningococcus PICU chapters at http://peds.stanford.edu/Rotations/picu/picu_rec_readings.html • • • • Cardiomyopathy Liver Failure Acute Renal Falilure Fluids, Electrolytes, Nutrition • Oncology • Transfusions • DKA • Submersion Injuries • Brain Death • End of life issues PICU Tables at http://peds.stanford.edu/Rotations/picu/picu_rec_readings.html • Sedation • Inotropes • Shock 2 Teams in PICU Team A Team B Attending Attending Fellow Fellow Second year pediatric resident Third year pediatric resident +/- NP ED resident Resident Role • Receive sign out from overnight resident • Pre-round on PICU patients • Present patients at morning rounds beginning promptly at 8:30am • After rounds carry out developed plan for each patient: e.g. call consults, follow up on radiologic studies, etc. • Discuss any management changes of patients with the attending / fellow prior to carrying out changes Resident Role • Be actively involved in stabilization of acutely ill patients • Evaluate new admissions to the ICU and develop a management plan • Present new admissions to the ICU fellow / attending • Attend evening rounds and transfer care of patients to overnight resident • Attend teaching conferences conducted by the ICU attendings / fellows Other Trainees in PICU • Anesthesia fellows • Emergency medicine residents • Medical Students Anesthesia Fellows • Present for half the blocks • Primarily provide support for fellow level activities in the ICU • Will not primarily follow patients ED Residents • Will act as a 5th resident in the PICU • May care for equal number of patients as pediatric residents • Rounds one day on weekend • Excused for Wednesday AM ED conferences: must pre-round & hand over notes to on call resident prior to leaving for education rounds Medical Students Primarily 2 rotations in PICU • Critical care core clerkship – all patients followed by students on this rotation must be co-followed by residents (most students on this rotation) • Sub-internship – these students can follow their own patients • Resident needs to write progress note PICU Evaluations for Pediatric Residents • Group faculty evaluation completed on Med-Hub • Verbal feedback from attendings while on the rotation – Be sure to illicit feedback if not provided Notes • The following need a full H&P: – – – – Trauma (even if went to OR first) Transport ED admits Direct admit from outside • The following need an accept note: – Post-op surgical – Transfer from floor/ rapid response Notes • Each patient needs PICU daily progress note (unless admitted in early am) • Significant events: codes/procedure/intervention – Require a note: confer with fellow who may do this note – Templates exist for most procedures • Interim summary weekly on Thursday for any patient with LOS > 5d in PICU Notes • • • • Online PICU specific templates Systems-based note Indicate attending on your team and select “sign” not “review” TIPS for PICU Notes • These are the official legal medical record • They support level of care provided • Therefore: – Avoid colloquials or not universally understood abbreviations – Use words to support ICU care— • instead of dehydration—mild tachycardia but stable, CR monitor • Try: dehydration with tachycardia, compensated shock in ICU for continuous hemodynamic monitoring ICU Transfers Requirements • Approval of the ICU Attending • Transfer summary – If going to a resident team, usually non-surgical and ICU stay >48h • Transfer orders – Surgical patients: surgeons often write orders – Always clarify with surgeon if OK to transfer & WHO will write transfer order • Sign patient out to ward resident Rounding & Presenting Patients Flow of Rounds • 8:30 Typically BMT, Liver, Renal Transplant • Followed by: – Sick/high acuity – Transfers – Remainder • Neurosurgeons round on their patients between 7:30-8:30 usually Tips for Success on Rounds • See CXR if available before rounds start…ETT high/low, new findings that can’t wait for rounds to start? • Any special drains in place? JP, Chest tube, EVD…know how much output total & per shift • Any pending studies completed from prior day? EEG, MRI, US, ECHO, cultures ….know the result • Patient identification • Quick assessment: i.e. patient improving, worsening, or unchanged • Major (not all) interval events • Vitals: Tmax (time) , vital sign ranges, including CVP, ICP if applicable Completing patient presentation • Be succinct; try not to present same data more than once • One line overall assessment of patient condition • Review orders • Address patient dashboard • Engage Bedside RN in rounds!! Procedures • PICU fellows are given priority for all procedures (particularly 1st year fellows) – Prerequisite for CCM training • Acute situations : fellow or attending Procedures Procedures residents should acquire some degree of comfort with while in the PICU • Bag-mask ventilation • Operating an anesthesia bag • Placement of peripheral IVs • Chest compression/Defibrillator familiarity • Code cart familiarity Bedside Nurses COMMUNICATION COMMUNICATION COMMUNICATION – Tell bedside nurse you are the resident caring for that patient – Give them your pager # Bedside Nurses Communicate all orders to the bedside nurse after written • Minimizes confusion about orders • Provides high level consistent patient care • Improves patient safety • Every nurse also has an Ascom phone if you can’t make it to bedside Bedside Nurses • The bedside RN = your eyes & ears to your patient • Provide “real time” clinical information • If they know what you are looking for – they can tell you - Especially with sick patients **They can make you look good by keeping you updated on all pertinent info! ** Orders • To minimize line entry RNs like to have flexibility to time meds – UNLESS You want drug given at a specific time – Qday ordered at 8pm won’t happen until 8 am next day • RNs may batch labs to minimize line entry *** except for immunosupression drugs *** e.g. Prograf, CSA Order Entry • Most routine labs and CXR require daily orders: – – – – CBC Coags Chemistries CXR • Qam labs in PICU are drawn at 4 or 5 am • TIP: Use PICU Daily Orderset during rounds!! PICU specific Power - Plans • In Cerner • PICU folder found under Power-plan folders PICU specific Power - Plans • On Cerner • Specific Powerplans available in PICU folder include: – – – – – – Fever work-up Trauma admit PICU Daily orders Respiratory failure DKA Hyperkalemia Admitting Trauma Patients • ANY TRAUMA patient—admit as follows: – – – – LOCATION: 2E/PICU Ward Attending: select PICU Attdg Service: Select Trauma (even if head trauma) Sub-specialty attending: Select Trauma or Neurosurgery Attending • If head trauma or NAT: Peds surgery/trauma must be notified to do tertiary survey • Trauma H&P in Epic, co-write admit orders Order Entry Reminders • Extubation: Requires an extubation order – Don’t just D/C vent order – Other important orders are linked to extubation • Blood product orders – Still require a call slip – Inform patient’s RN that products ordered • ACE(airway clearance evaluation) vs CPT – Allows some autonomy to RT to develop plan for best mode of therapy Discharges • • • • Patient safety dashboard useful tool! Prescription paper available from USA Loads into one printer and special tray Select the PICU prescription printer for all D/C scripts – Rx_picu_fntdsk PICU Quality and Safety • PICU Handoff Initiative for ALL OR Handoffs – One Message, One Time – Role cards utilized – IPASS tool for handoff comes with 45 min call PICU Quality and Safety • PICU Patient Safety Dashboard – Real time clinical decision support – Enhance patient safety and care coordination – Multidisciplinary- pulls from documentation in EMR – Bottom tab for each patient – Review at conclusion of rounds for EACH patient PICU Dashboard Tab ✔ ✔ Ensure Best Practices for ✔CABSI Prevention ✔Pressure Ulcer Prevention ✔VAP Prevention Discharge Planning Catheter Associated Bloodstream Infections Ventilator Associated Pneumonia Patient Safety COWS • Be sure to sign off • Don’t leave patient information exposed • Plug them back in (a dying cow is not pretty) • !! No cow tipping !!! PICU Etiquette • Please speak in quiet voices, particularly around main nurses station • We follow HUSH in the PICU Final Thoughts • • • • • Take ownership of your patients Be present Be involved Ask questions Suggestions on improving the rotation Questions, concerns, thoughts on the rotation Contact PICU rotation director Dr. Courtenay Barlow at cbarlow@stanford.edu Pager: 23492