Conjunctival Squamous Cell Carcinoma with Massive Intraocular
advertisement

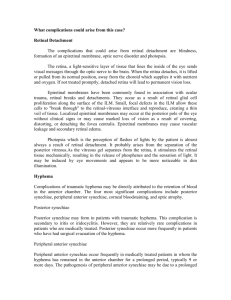
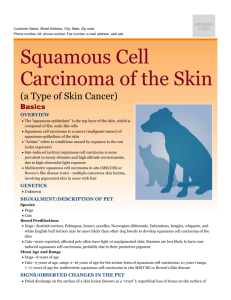
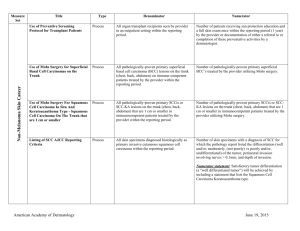
Conjunctival Squamous Cell Carcinoma with Massive Intraocular Invasion Fiona Roberts, Glasgow BAOP, Manchester 7-8th April, 2011 Clinical History • 75 year old male • 15 month history of left limbal mass • Biopsied Clinical History • Invasive poorly differentiated squamous cell carcinoma • Excision was considered best treatment However • Not a good 75 year old and generally frail • Decision to treat with topical mitomycin C • Review in 3 months 3 Month Review • Condition significantly deteriorated. • Struggling to open the left eye. • Vision had decreased from 6/24 to hand movement. • Mass had increased in size with dystopia • Rubeosis, posterior synechiae and an anterior uveitis. • No fundal view. • Pressure in the left eye was slightly raised Pathology CK14 Pathology Summary • Squamous cell carcinoma of the conjunctiva • Extensive intraocular spread – anterior chamber with malignant epithelial downgrowth and invasion of trabecular meshwork – Ciliary body – Choroid with mass forming posteriorly • Secondary effects of raised intraocular pressure Conjunctival Squamous Cell Carcinoma • Relatively uncommon worldwide • Geographical variation in incidence of 0.02 to 3.5/100,000 • Part of the spectrum of ocular surface squamous neoplasia (OSSN) • Occurs in sun-damaged ocular surface usually at the limbus in elderly males • Also associated with immunosuppression (AIDS, Transplant etc.) Intraocular Invasion of Conjunctival SCC • Reported to be rare (2 to 13% of cases) • Char et al. BJO, 1992 identified approximately 60 reported cases of intraocular invasion • Since then around a further 18 cases (13 as part of several series and 5 case reports) • Even been reported in a 12 year old Haflinger gelding Kaps et al. Veterinary Ophthalmology, 2005 Intraocular Invasion - Features • Most commonly in older patients with one or 2 recurrences Shields et al. 1999 • Tumour usually located near corneoscleral limbus • Heralded by onset of low-grade inflammation and secondary glaucoma • A white mass generally was observed in the anterior chamber angle • Most cases reported to date confined to anterior chamber and ciliary body and extension posteriorly is unusual Risk Factors 1 • Neglected primary malignancy – Did failure to excise primary tumour in this case equate with neglect ? – Topical mitomycin C is recognised as an effective treatment of SCC of the conjunctiva – Thin tumours less than 4mm can show complete regression even if extensive – Larger/thicker tumours may show only a partial response – Mitomycin C for chemoreduction prior to surgery Shields et al., Arch Ophthamol, 2005 Risk Factors 2 • Recurrent tumours/Inadequate primary excision – 73 year old male who had conjunctival SCC with intraocular invasion removed by corneoscleral resection with iridocyclectomy – Initial excision showed clear margins – Recurrence one year later in iris and trabecular meshwork well away from primary tumour Glasson et al., Arch Ophthalmol, 1994 Risk Factors 3 • Histological tumour type – Mucoepidermoid carcinomas • Lacour et al. J Fr Ophthalmol, 1991 • Seitz & Henke, Klin Monbl Augenheilkd, 1995 • Gunduz et al. Ophthalmology, 2000 – Spindle cell squamous carcinoma • Shields et al., Cornea, 2007 – Both regarded as more locally aggressive and to have a higher recurrence rate – However, each histological subtype accounts for few than 5% of squamous cell carcinomas of the conjunctiva Summary • Intraocular invasion from conjunctival squamous cell carcinoma is uncommon • Usually occurs in elderly males with mass at the limbus • Involves anterior chamber with signs of inflammation and raised intraocular pressure • Extension posteriorly is uncommon • Ocular prognosis is poor but survival is good