tef
advertisement

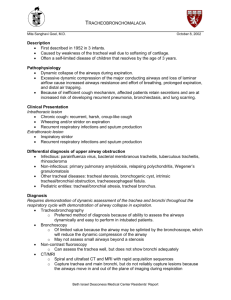
TRACHEOESOPHAGEAL FISTULA: • Tracheoesophageal fistula (TEF) is a common congenital anomaly of the respiratory tract, with an incidence of approximately 1 in 3500 live births TEF typically occurs with esophageal atresia (EA). Classification: Type C, which consists of a proximal esophageal pouch and a distal TEF, accounts for 84 percent of cases. TEF occurs without EA (H-type fistula) in only 4 percent TEF and EA are caused by a defect in the lateral septation of the foregut into the esophagus and trachea. The fistula tract is thought to derive from a branch of the embryonic lung bud that fails to undergo branching because of defective epithelial-mesenchymal interactions -associated anomalies in about half of the cases of TEF and EA, often as part of the VACTERL association • Clinical features: • polyhydramnios occurs in approximately two-thirds of pregnancies [89]. Additional clinical features relate to the presence of the VACTERL association • Infants with EA become symptomatic immediately after birth with excessive secretions that cause drooling, choking, respiratory distress, and the inability to feed. • A fistula between the trachea and distal esophagus leads to gastric distension. • Reflux of gastric contents through the TEF results in aspiration pneumonia and contributes to morbidity. • Patients with H-Type TEFs may present early if the defect is large, with coughing and choking associated with feeding as the milk is aspirated through the fistula. Dx • The diagnosis of EA can be made by attempting to pass a catheter into the stomach. • This finding can be confirmed with an anteriorposterior chest radiograph that demonstrates the catheter curled in the upper esophageal pouch. • When the diagnosis is uncertain or a proximal TEF is suspected, a small amount of watersoluble contrast material placed in the esophageal pouch under fluoroscopic guidance will confirm the presence of EA. R/x • surgical ligation of the fistula • isolated TEF is generally good • depends upon associated abnormalities. • Mortality rates for EA and TEF were greater for infants with associated cardiac disease • Complications after EA and TEF repair: anastomotic leak esophageal stricture and recurrent fistulae, gastroesophageal reflux and aspiration. Motility disorders and respiratory function abnormalities persist on long-term follow-up Types of tracheoesophageal fistulas Congenital tracheal stenosis Chest radiograph and CT scan of a tracheal diverticulum A) Chest radiograph displays a large right-sided rounded lucency at the base of the neck above the thoracic inlet. B) The CT scan confirms the nature of the lucency. It has the typical features of a tracheal diverticulum. TRACHEAL LESIONS TRACHEAL AGENESIS (aplasia or atresia) -rare condition -At birth, there is immediate respiratory distress, and affected infants die shortly after birth from respiratory failure. Diagnosis: trachea cannot be intubated despite adequate visualization of the larynx. TRACHEAL STENOSIS • Most commonly, tracheal stenosis presents as segmental stenosis anywhere along the trachea. • Clinical signs: retractions, dyspnea, inspiratory and expiratory stridor, hypercarbia, and hypoxemia. • Tracheal stenosis also should be considered in the differential diagnosis of recurrent, severe, or prolonged croup. • The diagnosis can be suspected by demonstrating a fixed intrathoracic obstruction pattern on inspiratory-expiratory flowvolume curves and confirmed by bronchoscopy, CT scan, or magnetic resonance imaging (MRI) scanning • • • • • • • • • • TRACHEOMALACIA AND BRONCHOMALACIA instability of the trachea or bronchi resulting from abnormally soft or pliable tracheal cartilages. With a delay in development of the supportive structures of large airways, excessive narrowing may occur during exhalation, Classification of the condition is based on the anatomic area that is involved (eg, tracheomalacia, tracheobronchomalacia, bronchomalacia). Clinical signs: stridor, wheezing, respiratory distress, and hyperinflation, either diffuse or localized. Cough is usually absent, and growth is not impaired disappear during sleep but become evident during agitation or respiratory infections. diagnosis is established by airway fluoroscopy or flexible fiberoptic bronchoscopy. in most patients, no specific therapy is indicated. In the most severe instances, supplemental oxygen, continuous positive airway pressure, tracheoplasty, or tracheostomy may be necessary. Recently, expandable stents have been inserted with some success.