Prediction of Adverse Outcomes in
Patients with Congestive Heart Failure
Meredith Brown/ Mentor Dr. Nan Smith-Blair
Funded by Arkansas Department of Education SURF Grant (2009)
Background and Significance
Congestive heart failure (CHF) - pathological condition in
which the heart is unable to pump the necessary volume
of blood to supply the body
As the efficiency of the heart’s pumping action declines,
vital organs are unable to receive the necessary oxygen
and nutrients found in the blood, and the functioning of
these organs declines
Progression of CHF is monitored by changes in certain
lab values and vital signs: BNP, HR, BP, SaO2
Background and Significance, continued
According to the AHA 2009:
CHF in the U.S. was estimated to have cost $39.2 billion in
2010
#1 reason for hospital admissions in those over the age of 65
Once diagnosed with CHF, 52% of individuals will die within 5
years
The number of any-mention deaths from HF was about the
same in 1995 (287,000) as in 2006 (283,000)
What has been done to detect changes in
CHF patients prior to an adverse outcome?
Retrospective Models: Acute Physiology and Chronic
Health Evaluation (APACHE) and the Mortality
Probability Model (MPM)
Real time computerized surveillance systems and rapid
response teams, such as the TREX system implemented at
WRMC
Current Need for Research
Lack of literature regarding the significance of the
magnitude of change (delta change) in relation to time of
various lab values and vital signs in the prediction of
adverse outcomes in this patient population
The implications of this research are possible future real
time monitoring systems that incorporate the significance
of the magnitude of change of certain values
Purpose and Aims
To identify factors present in CHF patients prior to the
development of an adverse outcome (transfer to ICU/CCU
and/or death)
Aim 1: To determine the magnitude of change in brain natriuretic peptide
(BNP), heart rate (HR), systolic blood pressure (SBP), diastolic blood
pressure (DBP), and arterial oxygen saturation (SaO2) in patients with a
diagnosis of CHF who experience an adverse outcome during their
hospitalization.
Aim 2: To determine the magnitude of change in BNP, HR, SBP, DBP, and
SaO2 in patients with the diagnosis of CHF who did not experience an
adverse outcome during their hospitalization.
Methodology
Patient Population: all adults admitted to an urban hospital in
NWA in 2009 with the diagnosis of CHF (excluding pediatric,
hospice, trauma, and pregnant patients)
Study Design:
Study protocol approved by U of A IRB (protocol number 09-11-252) and
hospital
Retrospective review of charts using a comparable number of
patients without an adverse outcome as generated by a random
sequencer
Data collection: initial weight (WT), BNP, HR, SBP, DBP, and SaO2
upon admission and for 24 hours prior to discharge or adverse
outcome
Data Analysis
One-way ANOVA with one between-groups factor design
was used to examine possible differences upon admission
and at the point of adverse outcome/no adverse outcome
between groups 1 (no adverse outcome) and 2 (adverse
outcome)
Two-way ANOVA with repeated measures on one factor
was used to analyze Group x Time interaction and delta
change on HR, SBP, DBP, and SaO2
Demographics
Sex
58.7% Males
41.3% Females
Age
range 29-94
< 65 years 27%
66-79 years 42.9%
> 80 years 30.2%
Race
2 Hispanic
1 Asian
58 Caucasian
Demographics
Variable
df
F Value
Significance
Sex
• 58.7% Males
• 41.3% Females
(1, 59)
0.04
p=.83
Age
• < 65 years 27%
• 66-79 years 42.9%
• > 80 years 30.2%
(1,59)
0.06
p=.81
Weight (Mean 85.5 kg; SD= 27.24)
• Group 1- 87.1 kg (SD 29.5kg)
• Group 2- 83.7 kg (SD 24.95 kg)
(1,59)
0.24
p=.63
RESULTS
One-way ANOVA with one between-groups factor design
Variable
df
F Value
Significance
Heart Rate (HR)
(11,42)
0.77
p= .77
Systolic Blood Pressure (SBP)
(11,42)
0.88
p= .57
Diastolic Blood Pressure (DBP)
(10,50)
1.46
p= .18
Saturation of Oxygen in Arterial
Blood (SaO2)
(11, 77)
1.0
p= .45
Blood pH (pH)
(1,16)
1.67
p= .21
Brain Naturiuretic Peptide (BNP)
(1,42)
13.75
p< .0006**
** Level of significance p < .05
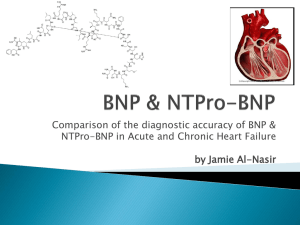
Brain Natriuretic Peptide (BNP)
*
M= 17,948.9 pg/mL
M= 5,535.7 pg/mL
*- p< .0006
Discussion: BNP
BNP = an “emergency hormone that responds immediately to
ventricular overload”
Rapid testing of BNP may be used in the future to guide
treatment of patients with decompensated CHF
Current AHA guidelines: do not yet recommend serial BNP
measurements to guide treatment
BNP affected by many variables: age, sex, weight, and renal
function
Call for further research in this area
Discussion: BNP
Anecdotally…
Group 1 = 33% of patients had slightly increased BNP
measurements over time (avg 24%)
Group 2 = 50% of patients had increased BNP measurements
over time (avg 64.6%)
One patient had a BNP of 11,264 pg/mL upon admission
(normal range is 0-100 pg/mL) that increased to 64,601 pg/mL
13 hours later
Call for continued research on the usefulness of serial BNP
measurements in predicting adverse outcomes
RESULTS
Group x Time interaction using 2-way ANOVA with
repeated measures on one factor
Variable
Df
F Value
Significance
HR
(11,42)
.77
p = .39
SBP
(11,42)
.88
p = .57
DBP
(10,50)
1.46
p = .18
SaO2
(11,77)
1.0
p = .45
No statistically significant delta changes noted in HR, SBP,
DBP, or SaO2
Discussion
Physiology of compensation (BP and HR)
Time of data entry not standardized possible masking
of important differences
May account for the lack of any identifiable trends – does
NOT rule out the possibility of clinical significance
Multiple factors to consider
RESULTS
One-way ANOVA with one between-factors design
at the point of adverse outcome/no adverse outcome
Variable
Df
F Value
Significance
HR
(1,58)
5.587
p = .021
SBP
(1,58)
2.220
p = .142
DBP
(1,58)
1.372
p = .246
SaO2
(1,59)
2.253
p = .139
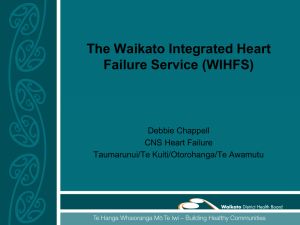
RESULTS: Heart Rate (HR)
*
*= Significance p = .021
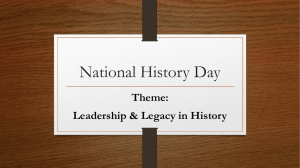
RESULTS: Systolic Blood Pressure (SBP)
==
RESULTS: Diastolic Blood Pressure (DBP)
RESULTS: Saturation of Arterial Oxygen(SaO2)
Call for further research and possible
clinical implications
Call for more frequent monitoring of HR
Possible serial measurements of BNP to track the progression
of CHF and to predict adverse outcomes
Standardized protocol for more consistent data which could
be analyzed for earlier detection of patient deterioration
Continued efforts to identify early indicators of adverse
outcomes in CHF patients due to the high morbidity and
mortality rates
References
1. Morton PG, Fontaine DK. Critical care nursing. 9th ed. Philadelphia: Wolters Kluwer Health and
Lippincott Williams & Wilkins; 2009.
2. Cheng V, Kazanagra R, Garcia A, Lenert L, Krishnaswamy P, Gardetto N, Clopton P, Maisel A. A rapid
bedside test for B-type peptide predicts treatment outcomes in patients admitted for
decompensated heart failure: a pilot study. J Am Coll Cardiol. 2001; 37: 386-391.
3. McDonagh TA, Cunnginham AD, Morrison CE, McMurray JJV, Ford I, Morton JJ, Dargie HJ. Left
ventricular dysfunction, natriuretic peptides, and mortality in an urban population. Heart. 2001; 86:
21-26.
4. Dunlay SM, Gerber Y, Weston SA, Killian JM, Redfield MM, Roger VL. Prognostic value of biomarkers
in heart failure. Circulation Heart Failure. 2009; 2: 393-400.
5. Melander O, Newton-Cheh C, Almgren P, Hedblad B, Berglund G, Engström G, Persson M, Smith
JG, Magnusson M, Christensson A, et al. Novel and conventional biomarkers for prediction of incident
cardiovascular events in the community. J of the Am Medical Association. 2009; 302(1): 49-57.
6. Ponikowski P, Anker SD, Chua TP, Szelemej R, Piepoli M, Adamopoulos S, Webb-Peploe, K,
Harrington D, Banasiak W, Wrabec K, et al. Depressed heart rate
variability as an independent predictor of death in chronic congestive heart failure secondary to
ischemic or idiopathic dilated cardiomyopathy. Am J of Cardiology. 1997; 79(12): 1645-1650.
7. Cleland JGF, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. The
effect of cardiac resynchronization on morbidity and mortality in heart failure. The New
England J of Medicine. 2005; 352: 1539-1549.
8. Mortara A, Bernardi L, Pinna GD, Spadacini G, Maestri R, Dambacher M, Muller C, Sleight P,
Tavazzi L, Roskamm H, Frey AW. Alterations of breathing in chronic heart failure: clinical
relevance of arterial oxygen saturation instability. Clinical Science. 1996; 91: 72-74.
9. American Heart Association. Heart disease and stroke statistics 2010 update: A report from
the American Heart Association. Circulation. 2010; 121: 46-215.
10. Gustafsson F, Torp-Pedersen C, Seibaek M, Burchardt H, Kober L. Effect of age on short and
long-term mortality in patients admitted to hospital with congestive heart failure European
Heart J. 2004; 25: 1711-1717.
11. Mosterd A, Cost B, Hoes AW, Bruijne MC, Deckers JW, Hofman A, Grobbee DE. Prognosis
of heart failure in the general population. The Rotterdam Study. European Heart J. 2001; 22:
1318-1327.
12. Senni M, Tribouilloy CM, Rodeheffer RJ, Jacobsen SJ, Evans JM, Bailey KR, Redfield MM.
Congestive heart failure in the community: trends in incidence and survival in a 10-year
period. Archives of Internal Medicine. 1999; 159: 29-34.
13. Stevenson LW, Braunwald E. Recognition and management of patients with heart failure.
Goldman L, Braunwald E. Primary Cardiology. Philadelphia, PA: W.B. Saunders; 1998.
14. Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA. Assessing
contemporary intensive care unit outcome: An updated Mortality Probability Admission Model
(MPM0-III). Critical Care Medicine. 2007; 35(3): 827-835.
15. Zimmerman JE, Kramer AA, McNair DS, Malila, FM. Acute Physiology and Chronic
Health Evaluation (APACHE) IV: Hospital mortality assessment for today's critically ill patients.
Critical Care Medicine. 2006; 34(5): 1297-1310.
16. Fu-Chiang T, Espino JU, Dato VM, Gesteland PH, Hutman J, Wagner M. Technical description
of RODS: A real-time public health surveillance system. J of the Am Medical Informatics
Association. 2003; 10(5): 399-408.
17. Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA,
Mancini DM, Rahko PS, Silver MA, et al. 2009 Focused update: ACC/AHA guidelines for the
diagnosis and management of chronic heart failure in adults. Circulation. 2009; 119: 1977-2016.