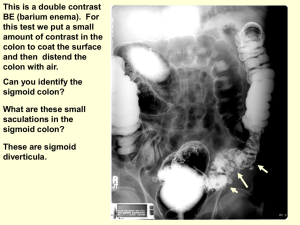
Air Contrast BaE
advertisement

Unit 5 Radiography of the Air Contrast BaE RDSC 233 Bontrager pp. 492-517 (air-contrast only) The Air-Contrast BaE Film Critique Positioning of: Rt. & Lt. lateral decubitus RAO & LAO obliques LPO axial (butterfly) Ventral decubitus rectum Upright-transverse Exposure Factors Radiographic Pathology The Air Contrast Barium Enema In the late 1970s the air contrast enema was introduced, and quickly became the examination of choice. An special air contrast enema tip provides for the introduction of air Coating the colon is done under fluoroscopy. First, thick barium fills the sigmoid and descending colon. Air, and patient positioning is used to push the column of barium to the cecum. Excess barium is drained back into the bag Retention balloon inflator Air inflator Barium tube The Air Contrast Barium Enema Four components that optimize the AC examination 1. Sufficient inflation of the colon 2. Thick barium to coat the bowel 3. Rolling the patient back and forth to keep the lumen coated. (Some routines require the patient to make a 3600 rotation in the middle of the filming routine) 4. Multiple positions, and extra projections to demonstrate every area of the bowel in the double contrast effect Radiographic Positioning of Additional Views for the Air Contrast Procedure Positioning of: Rt. & Lt. lateral decubitus RAO & LAO obliques LPO axial (butterfly) Ventral decubitus Upright-transverse including Film Critique Routine AC Colon Positioning Setup 1. 40” SID (relatively standard) 2. Reciprocating bucky 12:1, 16:1 grid 3. 80-90 kVp range 4. 14” x 17” film, lengthwise 5. ID marker at bottom 6. Rt marker above ID marker Routine AC Colon Positioning Preparation 1. Evaluate the order 2. Greet the patient 3. Take History What is pertinent Hx? Unlike the single contrast exam which may fail to demonstrate pathology of the mucosa of the bowel that is not ulcerated or significantly stenosed, the double contrast effect is preferred for the demonstration of polyps and small neoplasms 4. Remove jewelry, check attire, snaps, pins, NG tubes, etc. 5. Explain the exam in layman’s terms 6. Questions? 7. Set technique before positioning Routine Left and Right Lateral Decubitus Positioning Set up/Positioning Flash marker Same as for the abdomen decub. The grid & film is in a film holder. A horizontal beam projection to demonstrate the air-filled, bariumcoated half of the bowel on the side up. Sponge The right lateral decubitus position shown here, would result in a film that looks like this The patient is then rotated 1800 into the right lateral position Routine Decubitus Positioning Film Critique On all films Patient ID Rt or Lt marker Contrast & density Motion Artifacts 1. As much anatomy is included as can be included when well centered, primarily for the ascending and descending colon. 2. The bowel is sufficiently inflated 3. The air filled bowel is coated with barium Routine RAO & LAO Positioning Steps 350-450 obliques Entire spine (hips & shoulders) in same plane RAO: CR to iliac crest of side up (or slightly higher as indicated on observation of fluoroscopy) LAO: CR 2”-3” above iliac crest of side up (or significantly higher as indicated on observation of fluoroscopy) Critique Criteria for Anterior Colon Obliques Like posterior obliques (that are most commonly used in single contrast studies), anterior obliques are specifically designed to demonstrate the flexures. In AC studies all four oblique projections may be included in a routine. Inclusion of the sigmoid and rectum is usually not required The RAO is intended to lay the rt. colic flexure out in profile The LAO demonstrates the left Splenic flexure Routine AP Axial Oblique Positioning Steps In addition to the AP axial film, an AP axial projection combined with an LPO position may better separate the loop of the sigmoid. It may be used in a single contrast routine, but is frequently used for double contrast. 11” x 14” 300- 400 LPO CR 300- 400 cephalad CR centered 2” inferior, and 2’ medial to Rt. ASIS Criteria Include all of the sigmoid and rectum in an elongated view. Routine Ventral Decubitus Lateral Rectum Positioning Steps The ventral decubitus lateral rectum is a horizontal bean projection to further delineate the rectosigmoid area, in a double contrast effect. It is otherwise positioned like a lateral rectum. 10” x 12” or 11” x 14” CR at level of ASIS, mid coronal plane Criteria Include all of the sigmoid and rectum in an lateral, double contrast view. Routine Upright Positioning (Not in Bontrager) Setup and Preparation Same as an upright of the abdomen, except the film is usually used transverse. Positioning 4. Similar to an upright of the abdomen. Top of the film to the axilla, or at least high enough to include both flexures. Routine Upright Positioning (Not in Bontrager) Criteria The upright, transverse projection is designed to demonstrate the transverse colon in same manner the decubs demonstrate the ascending and descending. Note that the film seen here fails to meet the criteria for a good air contrast exam in the lumen of the transverse colon is not coated with barium due to: 1. Barium too thin 2. Insufficient coating before standing 3. Patient allowed to stand to long before exposure Exposure Factors From the “Rules of Thumb” 80 – 90 kVP Otherwise calculated from abdominal technique Significant Pathologies of the colon and their Radiographic Appearances Diverticulosis Abdominal hernias Tape worms Polyps Colorectal Cancer Chron’s disease Intussusception Institutional colon Septacemia – Pathogenic microorganisms in the blood. Ileostomy, jejunostomy, colostomy – ostomy = a surgically formed fistula, most commonly between intestine and the abdominal wall. (vs. otomy = surgical incision, vs. ectomy = removal) Stoma – A mouth like artificial opening between two body cavities, or a passageway between a cavity and a body surface Resection – partial excision of a part. Anastomosis – natural or surgical connection between two tubular structures. Glucagon – Hormone secreted by alpha cells of pancreas that stimulates liver to change stored glycogen to glucouse. Parentaral administration relaxes smooth muscles of alimentary tract. Diverticulum, Diverticulosis & Diverticulitis A diverticulum (singular) is a herniated outpouching in the wall of the colon. The occurrence of diverticula is diverticulosis. Inflammation of diverticula is diverticulitis. Caused by pressure on the bowel. Onset is usually over 40 years of age. Multiple diverticula of the sigmoid colon, seen in air contrast enema. A high-fiber vegetable diet lessens the incidence. Digested fiber passes more easily, due to its soft jelly-like texture. Diverticulum, Diverticulosis & Diverticulitis Symptoms * Abdominal tenderness * Nausea or vomiting * Chills or fever * Constipation or diarrhea BaE is the best imaging modality for demonstration of diverticula, though CT better detects abscesses. Several diverticula in the descending colon, seen on a single contrastBaE. Most diverticula are left sided, with the highest incidence in the sigmoid. Diverticula that perforate the colon cause peritionitis, a severe complication of diverticulitis Diverticulum, Diverticulosis & Diverticulitis Diverticula are most frequently seen in the colon, but can occur in hollow organs, primarily the stomach and bladder. This giant diverticulum of the colon is very rare. When bed-rest and antibiotics do not treat symptoms, or when extensive diverticula lead to fecal stasis, surgical resection of the most effected areas becomes necessary. Abdominal Hernia Protrusions of bowel may occur anywhere in muscular wall that contains it. Congenital defect, surgery, trauma, defective collagen synthesis, and strain (weight lifting, pregnancy, obesity) are contributing factors. Inguinal hernias are common in men, though not to the extent demonstrated here. Its prevalence is due to the weakened area of the pelvic floor where the testis pass from the pelvic cavity to the scrotum, through the inguinal canal. Tape Worm Though most prevalent in third world countries, intestinal parasites are found on occasion. Tape worms, of which there are numerous species, may be a few inches to to more than 50 feet. Hooks and suckers in the mouth part adhere to the intestinal wall. Body segments, which may number in the thousands, are immature, mature, and gravid: ending in segments containing mature eggs, that detach and are eliminated with feces. Tape Worm The life cycle of a tape worm After elimination by the host * Eggs develop into hooked embryo * Embryo are eaten by foraging animals, usually pigs or cattle (intermediate hosts) * Embryo develop as encysted larvae in muscle tissue * People ingest larvae in undercooked meat, and the cycle continues Symptoms include: bloating, discomfort, change in bowel habits, and if sufficiently infested, obstruction. Some species of larval cysts may incubate in the liver, pericardium, and brain. Polyps Typically, a benign growth of a highly vascularized mucosal lining classified as an adenoma. (Adeno=glandular, oma=tumor) Though asymptomatic, larger polyps can bleed. Some are pre-cancerous, and turn malignant. Sessile polyps are broad, slightly raised growths, that may have villous (tendril like) projections into surrounding tissue. Peunculated polyps are on a stalk, like a mushroom Among the many diverticula in this radiograph, is a pedunculated polyp Polyps Pedunculated polyp Similar polyp as seen on single contrast BaE Polyps Sessile polyp Sessile polyp (close up of) Colorectal Cancer Cancer is the uncontrolled reproduction of mutated cells, resulting in a useless mass of tissue called a tumor, malignancy, or neoplasm. Cancer of the colon occurs most frequently in the rectum and sigmoid, and is a leading cause of death. Shown here, is the classic look of an annular carcinoma (originating from epithelial tissue), commonly called an apple core lesion. Characteristics of growth Benign vs. Malignant Slow growth Undifferentiated ** Non-invasive Localized Rapid growth Highly differentiated * Highly invasive Metastatic * Cells, as seen on cytologic examination Colorectal Cancer An interesting comparison of an AP and PA projection: same patient, same exam, taken minutes apart. Note the changes in the position of the barium, and the demonstration of the apple-core lesion. Also, note the look of the pelvis Cancer Though colon cancer is most prevelant in the rectum and sigmoid, it may occur anywhere. Here, a polypoid mass invades the cecum, and involves the ileal papilla. Cancer of the colon is treated by surgery, chemotherapy, radiotherapy, or a combination of the three. Like all cancer, a cure is highly dependant on early detection and intervention before metastasis occurs. Crohn’s Disease Also called regional enteriitis, is one of two categories of inflammatory bowel disease, the other being colitis. Most commonly found in the terminal ileum, but can affect any part of the intestine. The cause is unknown, but, in theory, the body’s immune system, reacting to a virus or bacterium, inflames all layers of the bowel Symptoms Diarrhea Pain in the RLQ Radiographic appearance: Loops of Rectal bleeding bowel are separate due to inflammation. Weight loss Strictures create a characteristic “string Fever sign.” Ulcerations and edema create a Cramping “cobblestone” appearance. Stunted growth in children (though Chron’s is most prevalent between 20-40 years of age) Chron’s Disease In addition to the signs of Chron’s disease, something else shows, in what appears to be the sigmoid colon. What is it? T-shaped IUD Prognosis: Drugs control pain, inflammation, and bleeding; 70% of patients have surgery. There is no cure. Intussusception Telescoping, or slipping, of one section of bowel into another. Occurs chiefly in children, and at the ileocecal junction. In adults, intussusception may be secondary to a tumor or polyp. Mortality is high if left untreated for more than 24 hours. Intussusception Cecum Lateral projection of ileocecal intussusception Terminal ileum Intussusception 1. 3. An intussusception may be reduced by the pressure of a barium enema, instead of surgery. 2. 1. Barium reaching the cecum reaches the obstruction 2. Hydrostatic pressure reduces the defect. 3. Barium begins to reflux into the ileum, demonstrating success. Institutional Colon Preciously covered in Unit 1. The film on the left is an attempt to outline the impaction with contrast. The film on the right shows the result of a ruptured colon The end