Problem solving
A patient
with a clinical history
of hiatal hernia comes to the
radiology department. Which
procedure should be
performed on this patient to
rule out this condition? (5pts)
Problem solving
What
projection if the
radiograph of the stomach
demonstrates the fundus if
filled with contrast media and
the body and duodenal bulb is
filled with air with the lesser
curvature en face is best
visualized seen. Why? (5pts)
11.- 12. Two Types of Ileus
13. – 15 Division of the
small intestine
length
approximately
The
It begins
inisright
iliac region5
ft.
(152cm)
long
is greater
when
it joins
theand
ileum
of
in
than the small
thediameter
small intestine.
bowel.
Functions
The large intestine takes about 32 hours
to finish up the remaining processes of
the digestive system.
The large intestine simply absorbs
vitamins that are created by the bacteria
inhabiting the colon. It also absorbs
water and compacts feces, and stores
faecal matter in the rectum until
eliminated through the anus
Location
It starts in the right iliac region of the pelvis,
just at or below the right waist, where it is
joined to the bottom end of the small
intestine.
From here it continues up the abdomen, then
across the width of the abdominal cavity, and
then it turns down, continuing to its endpoint
at the anus.
Large Intestine Anatomy
CECUM
COLON
RECTUM
ANUS
Cecum
The cecum or caecum (from the Latin
caecus meaning blind) is a pouch,
connecting the ileum with the ascending
colon of the large intestine.
It is separated from the ileum by the
ileocecal valve (ICV) or Bauhin's valve,
and is considered to be the beginning of
the large intestine.
Ascending colon
The
ascending colon, on the
right side of the abdomen, is
about 25 cm long
It is the part of the colon from
the cecum to the hepatic
flexure (the turn of the colon
by the liver).
Transverse colon
The
transverse colon is the part of
the colon from the hepatic flexure to
the splenic flexure (the turn of the
colon by the spleen).
The transverse colon is encased in
peritoneum, and is therefore mobile
(unlike the parts of the colon
immediately before and after it).
Descending colon
The
descending colon is the part
of the colon from the splenic
flexure to the beginning of the
sigmoid colon.
The function of the descending
colon in the digestive system is
to store food that will be emptied
into the rectum.
Sigmoid colon
The sigmoid colon is the part of the
large intestine after the descending
colon and before the rectum.
The name sigmoid means S-shaped
The walls of the sigmoid colon are
muscular, and contract to increase the
pressure inside the colon, causing the
stool to move into the rectum.
*Rectum and Anal Canal*
Rectal
Ampulla
Anus
Anal
canal
Rectum
The rectum (from the Latin rectum
intestinum, meaning straight intestine) is
the final straight portion of the large
intestine and terminating in the anus.
The human rectum is about 12 cm long
Its caliber is similar to that of the sigmoid
colon at its commencement, but it is
dilated near its termination, forming the
rectal ampulla.
Colon subdivision
Ascending
Transverse
Descending
Sigmoid
Barium Enema (BE or Lower GI
series)
It is a Radiographic study
of the large intestine.
Purpose:
to study Radiographically
the form and function of the
large intestine, as well as to
detect any abnormal
conditions.
Clinical indications
Colitis
Diverticulosis
Neoplasm
Volvulus
Intussusceptions
Appendicitis
Colitis
Inflammation of the colon
Image – thickening of mucosal wall
and loss of haustral markings
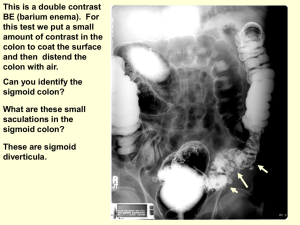
Diverticulum
outpouching of the mucosal wall
resulting from herniation of the inner
wall of the colon.
Image – jagged or sawtooth
appearance of the mucosa
Neoplasm
tumors in large intestine.
Image - narrowness or tapering of
lumen “apple core” or “napkin-ring”
lesions
Volvulus
twisting of a portion of the intestine
on its own mesentery.
Image – corkscrew in appearance
with air-filled distended region of the
intestine
Intussusceptions
telescoping of one part of the
bowel into another.
Image – mushroom-shaped
dilation at the distal aspect of the
intussusception with little or no
gass passing beyond it.
Colitis
Volvulus
“coffe bean”
Preparation of the Patient
The
final objective is that the
section of alimentary canal to
be examined must be empty.
2 – classes of Cathartics
(laxative)
Irritant cathartic – castor oil
Saline cathartic – magnesium
citrate or sulfate
Contraindications to Cathartics
Gross
bleeding
Severe diarrhea
Obstruction
Inflammatory lesions
(appendicitis)
Contrast Media
High
– density Barium Sulfate
It is excellent for use in double-
contrast studies of the alimentary
tract in which uniform coating of the
lumen is required.
Air
contrast
Carbon dioxide may also be used
because it is more rapidly absorbed
than nitrogen of air when evacuation.
Mixture of Barium suspensions
12
% - 25% weight /
volume – Single
contrast
75% - 95% weight /
volume – Double
contrast
Barium Containers
Closed
system type
enema
Open system type
enema
Close system type
Enema Tips
– common enema
tips
3
Plastic disposable
Rectal retention
Air contrast retention
Enema tips
Enema tips insertion
Sims position –
relaxes the
abdominal muscles
and decreases
pressure within the
abdomen.
Sims Position
Summary of Enema tip insertion
Describe the tip insertion to pt.
2. Place pt in sims position. (pt
should lie on the left side, with the
right leg flexed at the knee and hip
3. Shake and inspect the enema
container to provide good mixture.
Allow the barium to flow through
the tubing and from tip to remove
any air in the system
1.
Wearing gloves, coat enema tip
with water-soluble lubricant.(KY
jelly or any sterile lubricant)
5. On expiration, direct enema tip
toward the umbilicus proximally
1 to 1.5 inches
6. After initial insertion, advance up
superiorly and slightly anteriorly.
Do not force enema tip.
4.
Tape tubing in place to prevent
slippage. Do not inflate unless
directed by radiologist
8. Ensure IV pole/enema bag is
no more than 24 inches (60cm)
above the table. Ensure tubing
stopcock is in the closed
position and no barium flows
into the pt.
7.
Procedures
– Types of
Examinations of Colon
3
Single – contrast Ba.
Enema
Double – contrast Ba.
Enema
Defecogram
Defecogram
Cont…
Single
– contrast
utilizes only a positive
contrast medium.
Double
– contrast
Difference is that in an
examination there is both
air and barium.
Two-stage procedure described
“by Welin”
A. In which the entire colon is
filled with a barium
suspension.
B. Patient evacuates the
barium and immediately
returns to the fluoroscopic
table for injection of air or
other gaseous contrast into
the colon.
Single-stage double contrast
examination
The
barium and the air
are instilled in a single
procedure as compared
to the two-stage which
reduces time and
radiation to patient.
7 – pump method (by Miller)
1)
2)
3)
4)
5)
6)
7)
7 pumps, left lateral position
7 pumps, LAO position(left PAoblique)
7 pumps, prone position
7 pumps, RAO position
7 pumps, right lateral position
7 pumps, RPO position
+7 pumps, supine position
10 – Routine Sequence of
Radiographs
AP – Rectosigmoid area
Left lateral – Rectum
AP/PA – Full Barium whole
abdomen
4) AP/PA – Double Contrast
study
5) Left & Right Oblique –
Flexures
1)
2)
3)
Cont…
Left Lateral Decubitus – Air
Filled Colon
7) Right Lateral Decubitus – Air
Filled Colon
8) Pt. In Prone W/ Cross Table
Projection – Rectosigmoid
Area
9) Angle Prone – Rectosigmoid
6)