Musculoskeletal System - Catherine Huff`s Site

Musculoskeletal
System
Functions
Movement
Shape of body
Disruption of Function
Trauma
– Fracture
– Ligament Rupture
Degenerative disease
– Osteochondritis dissecans (OCD)
– Degenerative joint disease (DJD)
– Ununited Anconeal Process (UAP)
Disruption of function
Inflammation
– Myositis
– Panosteitis
Poor conformation
– Luxating patella
Neoplasia
– Osteosarcoma
Musculoskeletal Diseases
Usually painful, need analgesics
– Feel better, heal better, eat better, etc
Fractures
– Causes
Other traumas
Bone disease
Repeated stress
Barbaro
MS Diseases
Fractures
– Types
Open (compound) – broken skin
Closed – intact skin
Simple – 1 break
Comminuted –multiple pieces
Stable – ends apposed and fixed (ie greenstick)
Unstable
Compression
Fracture????
MS Diseases - Fractures
Signs
– History of trauma
– Pain or localized tenderness
– Lameness
– Deformity of bone
– Loss of function
– Localized swelling or bruising
Dx – X-rays
Fractures - Treatment
Stabilize joints above and below the fracture
External devices
– Splints
Permanent or temporary
Wood, metal, plastic, newspaper
Adequate padding – protect limb
Keep dry, decrease activity
Foul odor => necrotic tissue, infection
Swollen toes => too tight
Fractures – Treatment
Casts
– Plaster of Paris, fiberglass
– Permanent
Fractures: Fixation devices
Robert Jones bandage plastic splint metasplint application
Schroeder-Thomas splint
Fractures: Long Bone
External fixation
Fractures: Long bone
Rx
– Internal fixation devices
Intramedullary pin
– Provides good stability along axis of bone
– Rotation can be problem
– Removed after fracture heals
– Sterile surgical condition
Internal Fixation – Bone Plate
Comminuted fracture
Best stabilization
Should be removed after healing – most are not
Requires specialized instruments and surgery techniques
Provides early return to function
Fracture: Bone plate
Which bone? Where is fracture?
http://www.youtube.com/watch?v=
Wls_Pyop-D0&feature=channel_page
Bone Fractures – Client Info
Restrict activity
Watch for drainage, swelling, heat
Metal (plate, pin) stronger than bone
– refracture may occur
Follow up x-rays necessary
Metal should be removed after healing
Metal may cause cold sensitivity
Ligament Injury – Anterior Cruciate
Ligament
ACL and PCL (posterior cruciate ligament) stabilize knee joint
Intra-articular structures
Ruptured ACL – most common knee injury => DJD
May be complete rupture or partial tear => unstable joint => DJD
Anterior and Posterior Cruciate
Ligaments
ACL and PCL
Occurrence – sudden hyperextension or lateral extension of knee during exercise
Middle age, obese, inactive or highly athletic dogs; rare in cats
Sudden non weight bearing or limping
Swelling of knee joint
Rupture of contra lateral ACL often occurs within 1 year
Mensical tear often accompanies ligament tear
ACL – Dx
Anterior drawer movement
ACL – Repair
Surgical stabilization most successful
– Goal: stabilize knee to return function and minimize DJD
– Extra capsular stabilization
Most successful <30#
Suture material from flabella to tibial crest and imbrication of joint
ACL – Repair
Ligament rupture
http://www.youtube.com/watch?v=9 jg9E2nBt_E&feature=related
http://www.youtube.com/watch?v=4 nU2QZjjByg
http://www.youtube.com/watch?v=-
1pxxX4TXko&feature=fvw
ACL – Client info
Restrict activity 3-4 weeks post surgery
– Cage rest
– Leash walk only to urinate and defecate
Gradually increase exercise 4-8 wks post sx
Full activity 8-12 weeks
Opposite cruciate often tears within 1 yr
Weight loss helps
DJD of stifle joint likely
If no surgery, joint thickens - fibrosis
Patella Luxation
Grades
– I - Patella manually displaced but pops back into place
– II – Spontaneously or manually displaced till manually repositioned or patient extends stifle joint
– III – Patella luxated most of the time but can be manually replaced; movement of stifle joint reluxates patella
– IV – patella permanently luxated; unable to replace
Patella Luxation
Grades III and IV – crouching, bowlegged or knock-kneed stance for medial or lateral luxations, respectively
Pain: occurs as patella relocates or abrasion creates contact with bone
Patella Luxation
Patella Luxation
Medial Patella Luxation
Patella is in circle
Patellar groove indicated by arrow
Patella out of groove
Patella in groove
Patella luxation: Lateral
Seen in older dogs as the soft tissue of stifle deteriorates; often accompanies hip dysplasia
Produces more functional disruption than medial luxation
Clinical signs
– Acute lameness often associated with trauma or strenuous exercise
– Knock-kneed stance is sometimes seen
– If bilateral, animal may be unable to stand
Patella luxation: Medial
75% of cases
1 of most common stifle joint abnormalities in dogs
Bilateral involvement - 50% of cases
May occur in cats but not suspected, not lame
Clinical signs
– Usually bilateral
– Young (5-6 mo)
– Cow-hocked (knock-kneed)
– Foot twists laterally when weight bearing
– Skipping or intermittent hindlimb lamesness
Patella Luxation - Medial
Dx
– Toy and miniature dog breeds (yorkies,
Poms, Pekes, Chihuahuas, Boston terriers
– Palpate patella when knee is flexed
– X-rays show deformity and patellar displacement
Patella Luxation
Diagnostics
– Labs - ?
– X-rays – indicated for Grade III & IV luxations
– Arthrocentesis/synovial fluid analysis – minimal changes
Patella Luxation
Treatment
– I & II – outpatient treatment
NSAIDS – minimize pain, decrease inflammation
No steroids: SE and articular cartilage damage in long term use
+/- chondroprotective drugs – glucosamines, chondroitin sulfate
Patella Luxation
Treatment – II, III & IV –
– Surgical repair only option
Deepen trochlear groove
Tibial crest transposition for malalignment
Imbrication of joint capsule to stabilize patella in groove
Patella luxation: Repair
Rx
– Surgical repair is only treatment
(3 surgical options)
– 1) Deepen trochlear groove
Patella luxation: Repair
1A) Trochlear block resection (also deepens trochlear groove)
Patella luxation: Surgical repair
2) Transposition of tibial crest
Medial luxation patella
http://video.google.com/videosearch
?hl=en&q=patella+luxation+surgery
&um=1&ie=UTF-8&sa=N&tab=wv#
http://www.youtube.com/watch?v=G fnQbIk284g
Patella Luxation
Client info
– After Sx, limit exercise for 2-3 wk
– Support bandage (1-2 wk) should be kept dry
– NSAIDs for pain relief
– Ice pack for 5-10 min q 8 hrs for 3-5 days post surgery
– Physical therapy for rehab (swimming) helpful for animals reluctant to bear wt
– Will probably have some DJD later in life
Patella Luxation
Client Info
– May be inheritable
– Can worsen overtime esp without surgery
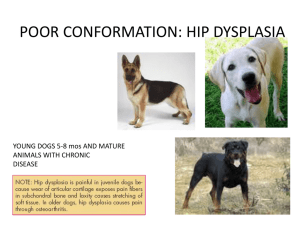
Hip Dysplasia
Def: Malformation and degenearion of the coxofemoral joint
Pathophysiology
– Developmental defect initiated by a genetic predisposition to subluxation of the immature hip joint
– Poor alignment between femoral head and acetabulum => abnormal forces on joint=> irregularly shaped acetabula and femoral head
– Also overload articular cartilage => microfractures and osteoarthritis
Hip Dysplasia
One of most common skeletal diseases in dogs
Incidence in cats lower that dogs
Breeds: Large breed dogs – St. Bernards,
G. Shepherds, Labs,
Golden Ret,
Rottweilers
Hip Dysplasia
Lowest prevalence are nearest in size to ancestral dog
Collie
– skin is tight, thin, smooth
Doberman
Collie
– slender/trim
Dalmatian
I Wolfhound
– muscles are full, hard
G Shorthair
– low fat % (1-2%)
– fleet footed, well-coordinated
Afghan hound
Belgium Tervuren
Siberian Husky
Incidence of HD
Highest prevalence
– giant breeds (2-3 x ancestral dog)
St Bernard
– bones are coarse and large Newfoundland
Bull mastiff
– feet are large and splayed
Eng Setter
– head is wide/oversized Gordon Setter
OE Sheepdog
– heavy, round, stocky
S Spaniel
– fat % (5-10% of ancestral dog) Akita
– muscles less developed
Ches Bay Retriever
G Retriever
– less graceful, slower Elkhound
Rott
– Grow/mature rapidly
G Shep
Within a breed, the faster growers are more prone to
HD
Pups of wolves, foxes are slow growing, late maturing vs dogs
Hip Dysplasia – Clinical Signs
Depends on degree of joint laxity, OA, and chronicity of disease
– Early – related to joint laxity
– Later – related to jt degeneration
– May present as early as 4-5 months
HX
– Decreased activity
Difficulty rising
Reluctance to run, jump, climb
– Intermittent or persistent hind limb lameness; worse after exercise
– Bunny hopping or swaying gait
– Narrow hind limb stance
Hip Dysplasia – PE
Pain on palpation of hips
Joint laxity (positive ortolani sign) – early disease – subluxation of hip
Crepitus
Decreased ROM of hip joints
Atrophy of thigh muscles
Hypertrophy of shoulder muscles
Hip Dysplasia
Dx
– X-rays provide definitive diagnosis
Quality depends on positioning, exposure technique, darkroom technique
– VD position
– Hind limbs extended fully and parallel
– Totally rotate legs medially
– Bilateral symmetry
– Flattening of femoral head,
– Shallow acetabulum
– Periarticular osteophyte production
– Thickening of femoral neck
Hip Dysplasia
OFA Certification
– Anesthesia/sedation usually required for positioning
– OFA requires animals to be >2 yr of age; 7 grades of hips
Excellent—near perfect hips
Good—normal
Fair—less than ideal, but within normal limits
Near normal—borderline conformation
Mild Dysplasia—minimal deviation with slight flattening of femoral head
Moderate Dysplasia—
Severe Dysplasia—complete dislocation of hip w/ flattening of acetabulum and femoral head
Hip Dysplasia: Normal hips
Normal hips
– round head except where lig of femoral head attaches
– Joint space (J) is consistent
Hip Dysplasia: OFA guidelines
Borderline —no consensus between radiologists to classify hip as Normal or Dysplastic
Good positioning
Normal dog
Poor positioning
1.
femurs not parallel
2.
Obturator foramen less rounded on R and wing of ileum larger on R
3.
R acetabulum appears shallower
4.
L acetabulum appears deeper
5.
Fabellae appear more medial to femur midline
6.
Wedge-shaped jt space due to lateral femoral rotation (looks like HD)
Hip Dysplasia
Penn Hip Registry – distraction radiography
Dorsolateral subluxation (DLS)
Dorsal acetabular rim view x-rays
Hip Dysplasia – Treatment
Medical
– Outpatient
– Analgesics and Antiinflammatories
Minimize joint pain=> use legs => decrease atrophy
– Does not correct problem; degenerative process progresses anyway
– Temporary relief of pain
– Carprofen, erodolac, deracoxib, tepoxalin
– Avoid corticosteroids – articular cartilage damage in long term use
– Do not combine NSAIDS
– Do not combine NSAIDS with steroids
– Wait several days when changing NSAIDs
– Glucosamine and chondroitin sulfate supplements chondroprotective
Hip Dysplasia – Treatment
Surgical
– TPO – triple pelvie osteotomy
6-12 months age
Preventive to correct alignment of joint
– Juvenile Pubic Symphysiodesis
Pubic symphysis fused early
Causes better alignment of acetabulum with femoral head
Can be done 3-4 months; minimal effect after 6 mo
Hip Dysplasia – Treatment
Surgical
– Total hip replacement
Salvage procedure in mature dogs with severed DJD unresponsive to medical Tx
Pain free in 90% of cases
Unilateral replacement provides acceptable function in 80% of cases
– Excision Arthroplasty or Femoral Head
Ostectomy
Forms “false” joint
Removal of femoral head and neck to prevent joint pain
Salvage procedure when medical treatment not working and other sx too expensive
Best - < 20#; good musculature
Abnormal gait
Total Hip Replacement and FHO
Hip dysplasia
http://www.youtube.com/watch?v=H
Twi8TRs6z8
Hip Dysplasia – Client Info
Weight control important to decrease load on painful joint
Swimming excellent activity
Physiotherapy – decreases joint stiffness, helps maintain muscle integrity
Joint degeneration progressive
May be heritable – do not breed
Special diets designed for fast growing dogs may decrease severity
Legg-Calve-Perthes Disease (LCP)
Spontaneous degeneration of the femoral head and neck leading to collapse of the coxofemoral joint and osteoarthritis
Avascular necrosis of femoral head and neck
Cause unknown
Infarction of the blood vessels of the proximal femur
Necrosis of subchondral bone => collapse and deformation of femoral head
Articular cartilage thickened, cleft development, fraying
LCP
Signalment
– Miniature, toy and small breeds, terriers
– 5-8 months old; range 3-13 mo
Clinical signs
– Lameness, gradual onset over 2-3 months
– Usually unilateral
– Pain on manipulation of hip
– Occasional crepitus in hip
– Atrophy of thigh muscles
LCP
Diagnosis
– X-rays
Early - Decreased bone density of epiphysis, sclerosis and thickening of femoral neck
Later- lucent areas in femoral neck
End-stage – flattening and extreme deformation of the femoral head, severe osteoarthritis
LCP
Legg-Perthes Disease
Collapse of femoral head 14 mo post-op FHO
LCP
Treatment
– Rest and analgesics
– Analgesics, anti-inflammatory drugs and cold packing 3-5 days post
– ROM exercises
LCP
Client education
– Recovery from surgery takes 3-6 months
– Glucosamines and chondroitin sulfate
– May be hereditary – do not breed
– With sx – good to excellent prognosis for full recovery
– Conservative therapy – alleviate lameness in 2-3 months in 25%
Osteochondrosis Dissecans (OCD)
Definition of osteochondrosis
– Pathologic process in growing cartilage, primarily characterized by a disturbance of endochondral ossification that leads to excessive retention of cartilage
– Ossification is slowed, cartilage thickens, is weaker and susceptible to stress, disrupts blood supply => necrosis of bone
– Osteochondrosis dissecans - Formation of a cartilage flap over the area of bone necrosis
– Bilateral disease common
– Most commonly affected joints: shoulder, elbow, stifle, hock
OCD: Pathology
OCD
Signalment: Large and giant breeds
– Great Danes, Labs, Newfoundlands, rottweilers, Bernese Mountain dogs,
Englishsetters, Old English sheepdogs
– Age: 4-8 months
Hx:
– Lameness – sudden or slowly increasing
1 or more limbs
Worse after exercise
Risk Factors:
– Diet with 3x rec levels of Ca
– Rapid growthand weight gain
OCD
PE:
– Pain on palpation or movement of affected joint
– Usually weight bearing lameness
– Joint effusion common
– Muscle atrophy if chronic
– Hock OCD- hyperextension of the tarsocrural jt
OCD: Shoulder m. atrophy
OCD – diagnosis
X-rays
– Flattening of subchondral bone or subchondral lucency
– Flap visualized if calcified
– Calcified bodies within the joint (joint mice)
Joint tap and analysis of synovial fluid
Arthroscopy
OCD: Dx
OCD: lesion
Great Dane humeral heads
OCD normal
OCD – Treatment
Early – no flap
– Restrict activity level
– Weight control
Flap (OCD)
– Surgical removal of flap or joint mice
– Antiinflammatories
– No corticosteroids
– Chondroprotective drugs (gluocosamine, etc)
OCD – Client Info
Heritibility – do not breed
DJD may develop even with surgery
Limit activity for 4-6 weeks
PT early on
Control weight
Restrict weight gain and growth in young dogs
OCD – Prognosis
Shoulder – good to excellent
Elbow, stifle, hock – fair to guarded
Panosteitis
Definition: a self limiting condition affecting one or more of the long bones of young medium to large breed dogs that is characterized clinically by high density of the bone marrow cavity
Cause unknown
Painful
May be one leg or become a shifting leg lameness
Panosteitis
Signalment
– Age – 5-18 months
– Dogs
Hx:
– No trauma
– Lameness of varying intensity
– Usually front legs but hind legs also
– Can be shifting leg lameness
– Severe: inappetance, weight loss, depression
Panosteitis
PE
– Pain on deep palpation of long bones in affected limbs
– +/- low grade fever
– +/- muscle atrophy
Panosteitis
Diagnostics
– X-rays: radiographic densities within the medulla of long bones
Normal density of bones
Panosteitis
Panosteitis
Panosteitis
Treatment
– NSAIDs- minimize pain; decrease inflammation
– Does not affect duration of disease
– Acetominophen not recommended
Panosteitis
Client Info
– Recheck q 2 weeks
– Self-limiting disease
– Treatment symptomatic
– Multiple limb involvement
– Lameness – few days to months
Luxations
Hip luxations are most common
Joint capsule must tear and ligament of femoral head must tear
Types
– Craniodorsal
most common
leg appears shorter
stifle rotates outward
– Cranioventral
Usually results from unsuccessful reduction of craniodorsal luxation
Stifle rotates inward
Leg appears longer
Hip Luxation
Signs
– Hx of trauma
– Acute lameness; non wt-bearing
– Possible swelling dorsal to hip joint
– Luxated limb shorter if legs extended in
VD position
Hip Luxation: Dx
Dx
– Thumb between greater trochanter—ischial tuberosity
Rotate femur away from body
– Disparity in leg lengths
– X-ray to r/o femoral neck fracture, Legg-Perthes
Hip Luxation
Hip Luxation
Rx
– Closed reduction
anesthesia required for proper muscle relaxation
– Using traction, rotate and pull head back in place
– Open reduction
Replace head of femur and suture soft tissue around acetabulum to keep it in place
– Either way, bandage in abduction x 2 wk (Ehmer sling)
Hip Luxation
Client info
– Px depends on:
Stability of the reduced joint
Soft tissue damage
Length of time prior to reduction of luxation
– Arthritis may occur
– Consider FHO/hip replacement if hip does not stay reduced
Luxation – Elbow
Less common
Difficult to reduce
DJD
http://www.youtube.com/watch?v=P
XMRDRetmgU
Myopathies
Def—Diseases of muscles
Inflammatory myopathies
– Bacterial myositis (dogs and cats)
Occurs following bite wd or contamination following
Sx
Usually Staphilococcus and Clostridium spp
– Protozoal myositis
Cysts form within muscles of Toxoplasmosis-positive cats
Myopathies Immune-mediated
Myopathies
Polymyositis—immune-mediated disease of dogs and cats
– Signs
Large breed dogs, middle-age
Weakness that gets worse with exercise
Stiff, stilted gait
Hyperesthesia on palpation
Fever, depression
Megaesophagus may develop (w/ aspiration pneumonia)
Muscle atrophy
Idiopathic
Dx—
– Elevated muscle enzymes (CPK)
– Muscle biopsy
Rx—Prednisone (2.2 mg/kg daily)
Myopathies
Immune-mediated Myopathies
– Masticatory muscle myositis (atrophic myositis, eosinophilic myositis)
Signs
– Involves muscles of mastication (temporalis, masseter)
These muscles have a special fiber type that has antigenic properties similar to antigenic properties of bacteria
– Muscles swelling initially
– Muscle atrophy and fibrosis
Acute Chronic
Rx—Glucocorticoids
Myopathies
Acquired myopathies
– Feline myopathy
Usually due to renal dysfunction and loss of K + in urine
Signs
– Cats of all ages, sexes, breeds
– Hypokalemia results in cervical ventroflexion
– Wt loss
– Periodic weakness, muscle pain
Rx—supplementation of potassium
Bone Tumors
Most bone tumors are osteosarcomas
(~100% malignant)
– Cause: unknown
– Signs (dist radius, prox humerus, dist femur, prox tibia)
Middle-age, large-breed dogs
Lameness
Wt loss
Pain, swelling of affected limb
Dx: x-rays show lysis/proliferation of new bone tissue
Bone Tumors
video
http://www.youtube.com/watch?v=t
88NK39rO_o
Bone Tumor
Dx
– Biopsy for definitive diagnosis
– Thoracic radiographs to r/o metastatic disease
Rx
– Amputation of affected limb
– Chemotherapy
– Radiation therapy
– No recommended drug therapies for cats
Client info
– Bone cancer is a fatal disease
– Survival time up to 12 mo with aggressive therapy
– Biopsy is needed to confirm diagnosis
– Amputation is necessary for comfort of animal, but it doesn’t affect likelihood of metastasis or survival
– Drug therapy and follow-up lab work are expensive
Declaw
Considered “inhumane” by some people
Outlawed in some European countries
San Francisco “advises” against it
It is an amputation of the last joint of cat’s toes
Declaw
Reasons why owners declaw cats
– Shredded furniture, drapes
– Scratched by cat
Procedure
– Apply tourniquet to leg
– Anesthetize, remove claws
– Tight bandages x 3 d
– Send home
Do not declaw outside cat
Dock Tails
Also banned in some European countries
Done at 2-5 days old
No anesthesia
1 stitch