Laryngo-tracheal Infections
advertisement

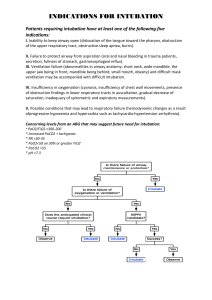
Laryngo-tracheal Infections Stridor It is the noise caused by obstruction of airflow due to narrowing in respiratory tract It may be inspiratory / biphasic /expiratory Inspiratory stridor alone indicates that the lesion is at vocal cord level or above An expiratory phase occurs when the tracheal lumen is also narrowed by oedema or inflammation Acute Laryngeal infections in childhood Acute Epiglottitis Laryngotrachealbronchitis Bacterial Laryngotrachealbronchitis Diphtheria Conditions which mimic laryngeal infections Acute Epiglottitis Most frightening pediatric emergency If unrecognized it can kill the child Haemophilus influenzae type B , is the causative organism in most cases The disease is concentrated maximally on the epiglottis but the inflammation may involve whole supraglottic compartment Most cases seen between 1 and 6 years of age, peak incidence between ages 3 and 4 Clinical features Sudden transformation of a fit child into one who is desperately ill, within a few hours Classical features: A fit child c/o sore throat which intensifies, with in half and hour dysphagia reported Inspiratory stridor develops and within 2 hours child becomes critical Child sits up and leans forward Saliva is dribbling due to absolute dysphagia Voice is muffled As time goes child becomes quiet and respiratory distress appears to lessen. An an ominous sign: respiratory & cardiac arrest imminent http://www.aic.cuhk.edu.hk/web8/epiglottitis%20picture.htm http://www.aic.cuhk.edu.hk/web8/supraglottitis.htm Management It is a surgical emergency Examination of throat by tongue depressor is particularly dangerous- sudden respiratory obstruction may occur Lateral X-ray of neck may show classical ‘thumb’ sign of swollen epiglottis If the clinical situation suggests that the diagnosis is epiglottitis , there is no point in confirming it what might turn out to be fatal X-ray www.learningradiology.com/archives04/COW%2010.. . The child is shifted to OT and anesthetized in upright position Laryngoscope inserted & diagnosis confirmed An appropriate size orotracheal tube inserted Otherwise rigid bronchoscope used to secure airway Tracheostomy / nasotracheal tube Culture swabs taken from epiglottis Nasogastric tube inserted for feeding I/V line established Best Clinical Practice Adults with suspected acute epiglottitis should be admitted and airway closely monitored Patients should be treated with I/V second- or third-generation cephalosporins and 100% humidified oxygen Airway obstruction should be treated early, ideally by intubation Laryngotracheobronchitis (Croup) As name suggests it involves larger proportion of respiratory tract Area of maximum impact is sub-glottis An acute illness with hoarseness, a barking cough, stridor and varying degree of respiratory distress Affects young children (6 months to 3 years) In most cases causative organism is paramyxovirus, para-infleunza virus type I and type II In adults it may also occur from herpes simplex, cytomegalovirus & influenza virus Adult croup is rare, more severe & impaired immunity should always be considered The key feature is sub-glottic oedema Investigations Direct viral antigen detection by sampling mucus from nasopharynx A plain neck radiograph may show narrowing of the subglottis (steeple sign) and ballooning of hypopharynx Chest X-ray to exclude collapsed lobes or meditational shift Management Oxygen, steroids and nebulized epinephrine should be administered Monitor airway and oxygen saturation, consider endotracheal intubation if necessary Broad spectrum antibiotics to cover secondary infection No evidence to support antiviral agents Best Clinical Practice Adult croup is rare but rapidly progressive Once suspected patient should be admitted Larynx inspected by flexible laryngoscope Broad-spectrum ABx to prevent bacterial infection If the airway deteriorates patient should be intubated and ventilated Bacterial Laryngotrachealbronchitis May be a separate disease or be caused by secondary bacterial infection of viral laryngotrachealbronchitis Also called bacterial tracheitis since it involves trachea predominantly Much more severe illness and much less common More severe respiratory obstruction and artificial airway is often needed Tracheostomy preferred over intubation Diphtheria Caused by Corynebacterium diphtheriae Spreads by droplet infection Affects non-immunised children and susceptible adults particularly elderly Usual site of infection is the tonsils and fauces but it can also occur in nasal cavities or spread to larynx Clinical Features Severe sore throat, malaise, pyrexia Examination of throat shows characteristic grey membrane in oropharynx which may spread to larynx Enlarged tender cervical lymph nodes Investigations A swab from throat for C/S A sample of grey membrane for screening Management Treat with benzyl penicillin and antitoxin Acute obstruction should be managed with intubation Complications: The diffusible exotoxin has predilection for cardiac and renal tissues Neurological complications soft palate paralysis, diaphragm & EOM Conditions which mimic laryngeal infections in childhood Foreign bodies Peritonsillar abscess Retropharyngeal Abscess Infectious mononucleosis Infectious mononucleosis A common disease often sub-clinical or mild Caused by Epstein-Barr virus Spread is usually transfer of infected saliva during kissing Clinical Features Acute sore throat with large infected tonsils Cervical lymphadenopathy with grossly enlarged bilateral lymph nodes Fever, Malaise There may also be palatal petechiae, oral ulceration, splenomegaly and hepatomegaly www.answers.com/topic/diphtheria Complications Gross swelling of tonsils and adenoids causes airway obstruction, but inflammation and ulceration can also extend to larynx The severity of laryngeal involvement may be masked by upper airway obstruction Splenic rupture CNS complications like encephalitis, meningitis, CN palsies Immune deficiency and HIV status be looked into Investigations Full Blood count Heterophil antibody test: Heterophil antibodies are antibodies that are stimulated by one antigen and react with an entirely unrelated surface antigen present on cells from different mammalian species Specific EBV serology HIV testing Management I/V fluids Analgesia In serious infections antibiotics, steroids and acyclovir should be considered Ampicillin / amoxycillin are best avoided for fear of inducing a maculopapular rash