ATLS - Trauma Overview

TRAUMA OVERVIEW
Mark E. Armstrong, M.D.
Overview
1. Preparation
2. Triage
3. Primary Survey
4. Resuscitation
5. Secondary Survey
6. Continued postresuscitation monitoring and re-evaluation
7. Definitive care
Preparation
Prehospital
Notify receiving hospital
Closest appropriate facility
Report pertinent information
Inhospital
Warmed IV solutions
Ancillary departments notified
Equipment made readily available
Hospital personnel protection
Primary Survey
A irway
B reathing
C irculation
D isability: Neurologic Evaluation
E xposure/Environmental Control
Primary Survey
Airway
Patency
Foreign bodies
Facial Fractures
Protect C-spine
Primary Survey
Breathing
Patency does not equal adequate ventilation
Expose chest
Auscultate
Conditions that may acutely impair ventilation
Tension pneumothorax
Massive hemothorax
Flail chest
Rib fractures
Open pneumo
Pulmonary contusion
Primary Survey
Circulation
Hemorrhage control
Two Key Elements
1. Level of Consciousness
-AVPU
-Glasgow Coma Score
2. Pulse
Bleeding
Control
No hemostats
Consider occult sources
Primary Survey
Disability
AVPU
Glasgow Coma
Verbal Response Motor response
Oriented 5 Obeys 6
Confused 4 Localizes 5
Inappropriate words 3 Withdraws 4
Incomprehensible sounds 2 Decortication 3
None 1 Decerebration 2
None 1
Eye Opening
Spontaneous 4
To speech 3
To pain 2
None 1
Primary Survey
Exposure
Remove all clothes
Cover to prevent hypothermia
Resuscitation
Airway
Oral
Nasal- do not put in someone with facial trauma
Endotracheal
Surgical
Breathing
Supply O2
Ventilate alveoli
Resuscitation
Circulation
Establish 2 large bore IVs
Draw blood
Vigorous IV therapy
ECG monitoring
Avoid hypothermia
Evaluate PEA
Other dysrhythmias
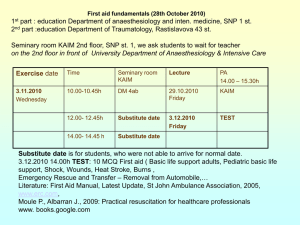
III
IV
I
Class
II
Hemorrhage classification
% blood loss
10 – 19
(750 cc)
20 – 29
(1250)
Heart rate
>100
Blood pressure
Slightly
Pulse pressure
Resp rate Capillary refill
Normal
Urine output
Delayed
30 – 39
(2000)
>40
>120
>140
(>30) Very
Delayed
Oliguria
Anuria
Other
Acidosis
Mortality
25%
60%
Resuscitation
Catheters
Urinary
Rectal first
Check for other signs of urethral injury
Gastric
Oral v.s. nasal placement
NGT Intracranial
Resuscitation
Monitoring
ABG ’ s
Pulse oximetery
Blood pressure
ECG
Roentgenograms
Should not delay resuscitation
AP pelvis
AP chest
Lateral C-spine
Odontoid, AP C-spine
Other Imaging
FAST scan
Focused Assessment Sonography in Trauma
Ultrasound
1.
Pericardial sac (epigastric area)
2.
Hepatorenal fossa
3.
Splenorenal fossa
4.
Pelvis or Pouch of Douglas (bladder)
Secondary Survey
Head-to toe evaluation
Vital sign evaluation
Detailed neuro exam if not done in primary survey
Special procedures
“ Tubes and fingers in every orifice ”
Secondary Survey
History
A Allergies
M Medications
P Past illnesses
L Last meal
E Events related to injury
1.Blunt
2.Penetrating
3.Burns
4.Hazardous Environment
Secondary Survey
History
A Allergies
M Medications
P Past illnesses
L Last meal
E Events related to injury
1.Blunt
2.Penetrating
3.Burns
4.Hazardous Environment
Secondary Survey (PE)
Head
Scalp
Eyes
Nose
Mouth
Bite occlusion
Secondary Survey (PE)
Head
PITFALLS
Hyphema
Optic nerve injury
Lens dislocation
Head injury
Posterior scalp laceration
Secondary Survey (PE)
Maxillofacial
Midline facial fractures
Bite occlusion
Bleeding
Fracture repair can wait
Midface Fractures
LaFort
I: Maxilla only transversely above the alveolar ridge
Most common isolated
II (pyramidal): Through nasal bone or nasal bone disarticulation with frontal bone
Most common when associated with other fractures
III (dislocated face): Through nasal bone, across floor of orbit, through lateral wall of orbit, zygomatic arch
Rare
Secondary Survey (PE)
Maxillofacial
PITFALLS
Pending airway obstruction
Changes in airway status
Cervical spine injury
Exsanguinating midface fracture
Lacrimal duct lacerations
Facial nerve injuries
Secondary Survey (PE)
C-spine and neck
Must be immobilized
Inspection
Palpation
Auscultation (carotids)
Secondary Survey (PE)
C-spine and neck
PITFALLS
C-spine injury
Esophageal injury
Tracheal or laryngeal injury
Carotid injury (blunt or penetrating)
Secondary Survey (PE)
Chest
Visual evaluation (ant & post)
Palpate rib cage
Sternal pressure
Auscultation (heart & lungs)
Chest xray
Secondary Survey (PE)
Chest
PITFALLS
Tension pneumothorax
Open chest wound
Flail chest
Cardiac tamponade
Aortic rupture (widened mediastinum)
Pneumothorax
Tension Pneumothorax
Secondary Survey (PE)
Abdomen
Frequently repeated exams
Inspection
Palpation
Normal initial exam does not rule out injury
Peritoneal lavage v.s. CT scan v.s. U/S
(FAST)
Secondary Survey (PE)
Abdomen
PITFALLS
Liver or splenic flexure
Deceleration injuries
Hollow viscus, Lumbar spine
Pancreatic injury
Major intraabdominal vascular injury
Renal injury
Pelvic fractures
Secondary Survey (PE)
Perineum/Rectum/Vagina
Contusions,Hematomas, Lacerations
Urethral bleeding
Rectal blood
High riding prostate
Sphincter tone
Vaginal vault injuries (pelvic fractures)
Secondary Survey (PE)
Perineum/Rectum/Vagina
PITFALLS
Urethral injury
Rectal injury
Bladder injury
Vaginal injury
Retrograde urethrogram
Secondary Survey (PE)
Musculoskeletal
Contusion
Deformity
Palpation
Pelvic pressure and compression
Vascular exam
Neurologic exam
Secondary Survey (PE)
Musculoskeletal
PITFALLS
SPINE FRACTURES
Fractures with vascular compromise
Pelvic fractures
Digital fractures
Secondary Survey (PE)
Neurologic
Immobilization of entire patient
Reevaluate GCS
Cranial nerve exam
Motor exam
Sensory exam
Monitor frequently for changes in neuro status
Assess O2 delivery if changes noted
Early neurosurgical consultation
Secondary Survey (PE)
Neurologic
PITFALLS
Increased intracranial pressure
Subdural hematoma
Epidural hematoma
Depressed skull fracture
Spine injury
Beware of unconscious patient
Subdural Hematoma
Epidural Hematoma
Aftercare
Continuous reevaluation
Definitive care