ATLS
advertisement

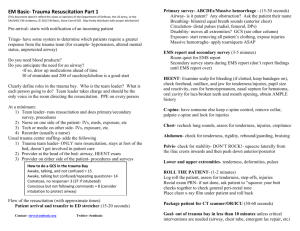
Chapter 1 Initial Assessment and management OBJECTIVES Identify the correct sequence of priorities in assessing the multiply injured patient Apply the primary and secondary evaluation surveys to assessment of the multiply injured patient Apply guidelines and techniques in the initial resuscitative and definitive--case phase Anticipate the pitfalls associated with the initial assessment and management ( minimize their impact ) Conduct an initial assessment survey on a simulated multiply injured patient CONCEPTS OF INITIAL ASSESSMENT Preparation Triage Primary survey ( ABCDEs ) Resuscitation Adjuncts to primary survey and resuscitation Secondary survey ( head-to-toe evaluation and history ) Adjuncts to the secondary survey Continued postresuscitation monitoring and reevaluation Definitive care Repeat primary and secondary survey when finding any deterioration in the patient’s status Primary survey and resuscitation are done simultaneously PREPARATION Prehospital – Airway maintenance – Control of external bleeding & shock – Immobilization of the patient – Communication with receiving hospital & immediate transport to the closest, appropriate facility – History taking ( include events ) Inhospital – Advanced planning ( especially massive casualty ) – Equipment & personnel – Communicable disease protection – Transfer agreements TRIAGE Sorting of patients according to ABCs and available resources Triages is the responsibility of prehospital personnel Not exceed the ability of the facility ==> treat life -threatening patient first Exceed the capacity of the facility ( mass casualties ) ==> Treat the greatest chance of survival, with the less time, less equipment & less personnel PRIMARY SURVEY Adult / Pediatric priorities same Identified the life-threatening conditions and simultaneously managed – A: Airway maintenance with cervical spine protection – B: Breathing and ventilation – C: Circulation with hemorrhage control – D: Disability ( Neurologic status ) – E: Exposure / Environmental control: Undress the patient & prevent hypothermia PRIMARY SURVEY Airway Maintenance with Cervical Spine Protection – Oral foreign bodies, facial, mandibular, or tracheal / laryngeal fractures may result in airway obstruction – Assume C-spine injury Multisystem trauma Altered level of consciousness Blunt injury above clavicle – Pitfalls: Difficult airway Obesity: surgical airway cannot be performed smoothly laryngeal fracture or incomplete upper airway transection PRIMARY SURVEY Breathing and Ventilation – Airway patency adequate breathing & ventilation – injury that may acutely impair ventilation 1. Tension pneumothorax 2. Flail chest with pulmonary contusion 3. Massive hemothorax 4. Open pneumothorax above problems need to be identified in the primary survey and managed – Pitfall: Differentiation of ventilation problems from airway compromise may be difficult PRIMARY SURVEY Circulation with Hemorrhage Control – Assess blood volume and cardiac output level of consciousness skin color pulse – Bleeding control: direct manual pressure on the wound – Pitfall: The response of elderly, children, athletes and others with chronic medical conditions to hypovolemia is different from normal people PRIMARY SURVEY Disability ( Neurologic Evaluation ) – Level of consciousness A. Alert V. Response to voice P. Response to pain U. Unresponsive – Pupils – Pitfall: Lucid interval ( talk and die ) : EDH, frequent neurologic reevaluation can minimize this problem PRIMARY SURVEY Exposure/Environmental Control – Undress patient completely – Protect from hypothermia – Pitfall: early control of the hemorrhage is the best method to keep body temperature( early surgical intervention) RESUSCITATION Protect/Secure airway & protect C-spine Breathing/Ventilation/Oxygenation Vigorous shock therapy – At last two large - caliber IV line – Crystalloid solution ( Ringer’s lactate 2~3 litter) – Type-specific blood – surgical intervention Protect from Hypothermia : 39oC warm IV fluid Urinary/gastric catheters unless contraindication ADJUNCTS TO PRIMARY SURVEY AND RESUSCITATION Monitor: – Ventilatory rate and ABGs/ end-tidal CO2 Pitfalls: Combative patients often extubate or bite endotracheal tube – Pulse oximetry – ECG & BP monitor – Temperature – urine output X-RAY AND DIAGNOSTIC STUDIES Can’t delay or interrupt the primary survey and resuscitation Trauma series ( portable X-ray ): CXR, C-spine/ lateral view, pelvic AP view A negative or inadequate c-spine x-ray can’t exclude cervical spinal injury Sonography / DPL Pitfalls: obesity ( Sonography and DPL are difficult ) CONSIDER NEED FOR PATIENT TRANSFER Referring doctor -to -receiving doctor communication Closest appropriate hospital BEFORE SECONDARY SURVEY Complete primary survey Establish resuscitation Normalization of vital functions SECONDARY SURVEY History taking Complete neurologic exam. Head-to-toe evaluation Roentgenograms Special procedure Tubes and fingers in every orifice Re-evaluation SECONDARY SURVEY History – A. Allergies – M. Medications currently used – P. Past illness / pregnancy – L. Last meal – E. Events / Environment related to injury HISTORY Mechanisms of injury Blunt – Automobile collisions Seat belt usage Steering wheel deformation Direction of impact Ejection of passenger form the vehicle Burns and Cold injury – Inhalation injury and CO. intoxication in fire field Hazardous environment Penetrate – Anatomy factors – Energy transfer factor Velocity and caliber of bullet Trajectory Distance SECONDARY SURVEY Physical Examination – Head – entire scalp and head – eye: pupil visual acuity EOM foreign body ( soft contact lens….) – Pitfalls: Severe facial swelling or unconsciousness p’t still need eye exam. SECONDARY SURVEY Physical Examination – Maxillofacial No airway obstruction or massive bleeding ==> treat later Midfacial fracture ==> R/O cribriform plate fracture Pitfalls: Some facial bone fracture is difficulty identified early ==> reassessment is crucial SECONDARY SURVEY Physical Examination – C-spine and Neck Maintain immobilization Complete evaluation Complete radiology study Cautions helmet removed Penetrating injury: Not be explored in the emergency department; explored & treat in the operative room Pitfalls: Blunt injury to Neck: Carotid artery intima injury or dissection ( delay onset ) Immobilization ==> decubitus ulcer SECONDARY SURVEY Physical Examination – Chest Pitfalls: – Poor tolerance to minor pulmonary trauma in elderly patients – A normal CXR can’t role out chest injury in children SECONDARY SURVEY Physical Examination – Abdomen Identify a surgical abdomen is more important than doing a specific diagnosis ==> early consult surgeon Close observation & frequent reevaluation of the abdomen DPL, sonography, abdomen CT Pitfalls: – Excessive manipulation of the pelvis should be avoid ==> just do pelvic x-ray – Retroperitoneal organs ( pancreatic & hollow organ ) are very difficult to identify SECONDARY SURVEY Physical Examination – Perineum / rectum / vagina Perineum: Contusions, hematomas, urethral bleeding……. Rectum: Sphincter tone, high riding prostate, blood….. Vagina: Blood, laceration Pitfalls: Female urethral injury is difficult to detect SECONDARY SURVEY Physical Examination – Musculoskeletal Extremities / pelvis: Contusion, deformity, pain crepitation, abnormal movement Vascular: Assess all peripheral pulses Spine: Physical findings, mechanism of injury SECONDARY SURVEY Physical Examination – Neurologic Determine GCS score Re-evaluate pupils Sensory / motor evaluation Maintain immobilization Prevent secondary CNS injury ( keep stable vital signs, avoid increased ICP and treat IICP ) Early neurosurgical consultation Pitfalls: Intubation should be done expeditiously and as smoothly as possible ( Intubation will increase ICP ) REEVALUATION New findings / deterioration / improvement High index of suspicion ==> early diagnosis & management Continuous monitoring Pain relief DEFINITIVE CARE Trauma center Closest appropriate hospital RECORDS AND LEGAL CONSIDERATIONAS Records: Concise, chronologic documentation Consent for treatment Forensic Evidence: preserve the evidence SUMMARY Initial assessment & management of multiply injured patient Primary survey ( ABCDEs ) Resuscitation & monitor ( life-threatening problems ) Secondary survey ( head-to-toe, history ) Definitive care ( early consultation, surgical intervention or transport )