DEBATE?
THERE IS NO
DEBATE
Traditional Perioperative Care
•Starve
•Stress
•Drown
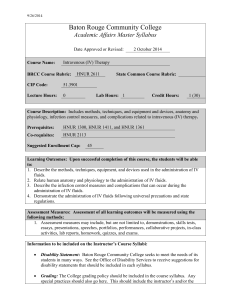
Functional capacity
Enhanced recovery after surgery
Surgery
Multi-modal intervention
Traditional care
Days
Weeks
KCH Fearon 2004
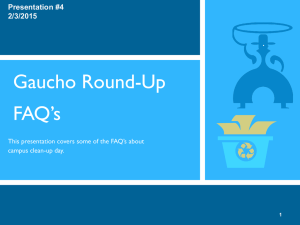
PATIENT’S JOURNEY
C
L
I
N
I
C
Surgery
Preop
↨
Anesthesia
H
D
U
Ward
Audit of compliance & outcomes
Home
Core Protocol
Audit of compliance/
outcomes
Preadmission
counselling
Selective bowel-prep
Perioperative
oral nutrition
CHO- loading/no fasting
No - premed
Early removal of
catheters/drains
No NG tubes
ERAS
Stimulation of
gut mobility
Short-acting
Anaesthetic agent
Prevention of
nausea and vomiting
Non-opial oral
Analgetics/NSA ID`s
Standard
mobilisation
Thoracic epidural
Anaesthesia
Avoidance of
Sodium/fluid overload
Short incisions
Warm air body
heating in
theatre
FLUIDS
FOOD
RESUSCITATION
WET IS BEST
ELECTIVE SURGERY
BALANCED IS
BETTER
KCH Fearon 2004
Post-op Weight Gain
Following Colorectal Resection
3-6kg
Lobo et al, Lancet
359: 1812-18
Brandstrup et al, 2002;
Annals Surg 2003; 238: 641-8
Hypothesis
Fluid/Saline
Overload
Hypoalbuminaemia/Acidosis/Hyperchloraemia
Gut oedema/Malfunction
Delayed recovery
Effect of salt and water balance in recovery of
gastrointestinal function after elective colonic
resection
20 colonic resection
patients
10
Standard IV
fluids
10
Restricted IV*
fluids
(* 2l H20 and 77mmol NaCl)
Lobo et al, 2002
Lancet; 359: 1812-8
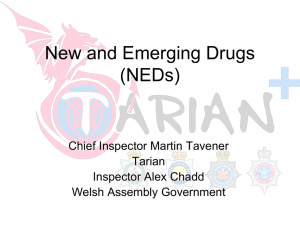
Effect of fluid and salt restriction in
post-op recovery
Standard Group
Restricted Group
4
3
2
p<0.0001
1
0
Standard Group
Restricted Group
40
-1
Serum albumin (g/L)
Change in weight (kg)
5
p=0.01
35
30
-2
0
1
2
3
4
Postoperative days
5
25
Preop 1
2
3
4
Postoperative days
5
6
Effect of fluid and salt
restriction in post-op recovery
200
200
n=10
n=10
n=10
p=0.028
150
100
50
0
Standard
Group
Restricted
Group
Liquid phase gsric emptying
time T50 (min)
Solid phase gastric emptying
time T50 (mm)
250
150
n=10
p=0.017
100
50
0
Standard
Group
Restricted
Group
Post-op Fluid Management
OPERATION
POST-OP
2-4d
4-6L
TRADITIONAL
2-3L
1-2d
BALANCED
2-3L
1-2L
What is the evidence base
to suggest that
BALANCED fluid
management can
improve outcomes?
Effects of IV fluid restriction on
post-op complications
172
Colorectal resection
patients
86
Standard IV
fluids
86
Restricted IV
fluids
72
competed
69
completed
Brandstrup et al,
2003; 238: 641-8
Number of Patients with Complications
(Per-Protocol Analysis)
Blinded Assessment
Restricted
Group
Standard
Group
p value
Overall complications
21
40
0.003
Major complications †
8
18
0.040
Minor complications †
15
36
0.000
Tissue-healing complications †
11
22
0.040
Cardiopulmonary complications †
5
17
0.007
Effect of Intra-operative Fluid Management
on Outcome after Intra-abdominal Surgery
Randomised
n=152
n=75
n=77
Liberal regimen
(Bolus 10ml/kg followed
By 12ml/kg/hr)
Restricted regimen
(4ml/kg/hr)
P
Intra-op
3.8 ± 1.2 L
1.4 ± 1.0 L
<0.001
Day 1
2.0 ± 0.5 L
2.2 ± 0.5 L
N.S.
Day 2
2.0 ± 0.5 L
2.1 ± 0.5 L
N.S.
Day 3
1.9 ± 0.5 L
2.0 ± 0.5 L
N.S.
Nisanerich et al 2005, Anaesthesiology; 103: 25-32
Effect of Intra-operative Fluid
Management on Outcome after Intraabdominal Surgery
Outcome
Restricted Liberal
P
No. of pts with
complications
Length of stay (d)
13
23
<0.05
8
9
<0.01
Moved bowels (d)
4
6
<0.001
Nisanevich et al 2005, Anaesthesiology; 103: 25-32
If you Limit Intra-operative Fluids
(10ml/kg/hr), does Early Discontinuation of
IV Fluids Influence Outcome?
Colorectal
n=80
n=41
STANDARD
n=39
LIMITED
3L H20/d
154mmol Na/d
3d
2L H20/d
60mmol Na/d
1d
Makay et al
(sumbitted)
Effect of Restricted Intra-op
Fluids Plus Discontinuation of IV
Fluids on Day 1
Restricted ‘Liberal’
P
No of complications
14
10
NS
Length of stay (day)
6
6
NS
Moved bowels (day)
4
4
NS
Makay et al (submitted)
BALANCED
IS
BEST
Postoperative early enteral nutrition
Lewis BMJ 2001
Traditional Care Day1
ERAS Day1
Effect of ERAS on spontaneous oral diet
Food intake
kcal / 24h
1600
1200
800
400
0
1
2
3
4
Postop days
Nygren Clin Nutr 2003
traditional care
enhanced-recovery protocol
Complications, length of stay and readmissions
within 30 days of colorectal resection
ERAS
n = 425
Traditional*
n = 451
Anastomotic leak %
4.2
3.9
Mortality %
1.2
1.5
5
8
Actual length of stay (days) (median)
P
<0.01
* Nygren et al Clin Nut 2005;24:455-461
ERAS GROUP
THE END
 0
0