Emergency Contraception (EC)
Emergency
Contraception
Clinical Effectiveness
Unit
August 2011
http://www.fsrh.org/pdfs/CEUguidanceEmergencyContraception11.pdf
Emergency
contraception (EC) is
a method of
preventing pregnancy
following unprotected
sexual intercourse
(UPSI) or potential
contraceptive failure.
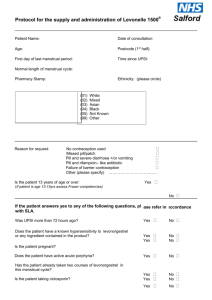
Minimum history required
• Pharmacists can do this so……..
Minimum history required
• LMP
• Cycle length (shortest)
• When did they have sex? Including prior
episodes in current cycle and any EC?
• Drug history
• Allergies
• Would a pregnancy be disasterous?
3 options
• Copper Intrauterine device (IUD)
• Levonorgestrel 1.5mg (Levonelle One
Step or Levonelle 1500) LNG
• Ulipristal Acetate 30mg (ellaOne) UPA
Timing and efficacy
Copper IUD
Failure rate considerably lower than 1% and not affected by timing
(1963 women and no pregnancies in first month)
Can be fitted up to120 hours after first episode of UPSI or up to 120
hours from the earliest estimated date of ovulation
A Cu-IUD can be fitted in good faith, providing appropriate steps have
been taken to try and establish earliest estimated date of ovulation
Timing and efficacy
LNG
Incompletely understood action ?inhibits ovulation
May delay ovulation by 5 days
No better than placebo at suppressing ovulation when
given immediately prior to ovulation
Licensed for 72 hours. May be effective up to 96 hours.
Quicker the better. Cycle timing probably alters efficacy.
Can be used more than once in cycle (If more than 3
weeks - pregnancy test first)
Timing and efficacy
UPA
Licensed up to 120 hours after UPSI
Thought to inhibit or delay ovulation
No apparent decline within that time period
Glasier study 2010 randomised, non-inferiority trials
showing UPA no less effective and non-significant trend
towards lower pregnancy rates with UPA
Should not be used more than once in cycle or if there has
been another episode of UPSI outside 120 hr window
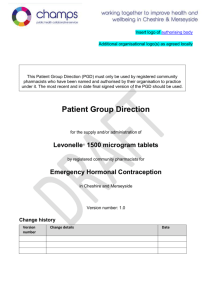
Pregnancy Rate by 24hr
3.03%
2.97%
2.74%
2.55%
2.13% 2.19%
1.60%
UPA
LNG
1.48%
0%
0-24h
25-48h
49-72h
73-96h
0%
97-120h
Copper IUD
Can be fitted up to 120 hours after first
episode of UPSI
Can be fitted up to 120 hours after earliest
estimated date of ovulation
Intrauterine device (IUD)
Not suitable for?
Acute PID
Patients who would not tolerate speculum examination or fitting
procedure
Risks
Failed fitting
Uncomfortable to fit
Perforation 1-2 in 1000
Expulsion 1 in 20
Ectopic pregnancy
Infection (increased risk in first 20 days)
Periods may be heavier or longer in first 3 months
Cu IUD
A Cu IUD should be offered to all women
requesting EC if timing is appropriate
If it is not possible to insert Cu IUD at first
presentation oral EC should be given in
the interim in case she changes her mind
or it is not possible to fit the IUD.
Restrictions for oral EC
LNG
Liver–enzyme inducing
drugs
Outside product licence
give double dose 3mg
UPA
Liver-enzyme inducing
drugs
Drugs that increase
gastric pH
Severe asthma controlled
by oral glucocorticoids
Hepatic dysfunction
Breastfeeding (36 hours)
Investigations?
STI screen including HIV
Window period
Consider antibiotics for emergency IUD
eg.azithromycin 1g PO
ceftriaxone 500mg IM dissolved in 2mls 1% lidocaine
Hepatitis B vaccinations
Additional Contraceptive
Precautions Required
EC option
COCP
POP
QLAIRA
LNG
7 days
2 days
9 days
UPA
14 days
9 days
16 days
The Qlaira pill pack
When should EC be used?
•
•
•
•
•
•
When no contraceptive method used
Following sexual assault
Split or slipped condom
Forgotten progestogen only pills
Forgotten combined pills or patch or ring
When depo provera late
Indications for EC
POP
>27 hours since last POP and UPSI in next
48 hours
>36 hours since last desogestrel only pill
and UPSI in next 48 hours
Depo-provera
Late injection (>14 weeks) and UPSI after
this time.
Indications for EC
COC
Missed two or more active pills
AND these are in the first week of packet
AND UPSI in the first week of taking pills or
pill free interval
Menopause
If under 50 years – need 2 years of
contraception from LMP
If over 50 years – need 1 year of
contraception from LMP ……..
If amenorrhoeic due to POP or Mirena use
FSH levels to determine “LMP”