Antifungal management in the haematology patient
advertisement

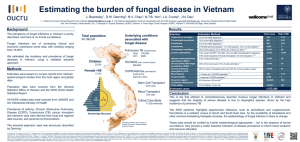
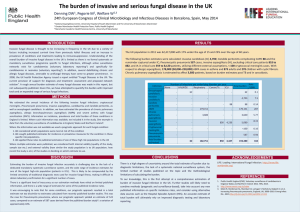
Antifungal management in the haematology patient David W. Denning University Hospital of South Manchester The University of Manchester Treatment Invasive aspergillosis IDSA guidelines. Walsh et al. Clin Infect Dis 2008;46:327 Invasive aspergillosis Why most and not all? IDSA guidelines. Walsh et al. Clin Infect Dis 2008;46:327 Arguments for not using voriconazole 1. Amphotericin B is a broader spectrum agent Frequency of mucormycosis in leukaemia 391 pts with leukaemia (225 with AML) and a filamentous fungal infection 80% neutropenia for >14 days, and 71% neutropenic at time of diagnosis 85% pulmonary infection Antemortem diagnosis in 79% Aspergillus 296 (76%) Mucorales 45 (11.5%) Fusarium 6 Other 4 Unidentified in 40 Overall mortality in 3 months 74%, 51% attributable Pagano et al, Hemtaologia 2001;86:862 Intrinsic and acquired resistance among the Aspergilli Amphotericin B resistance A. terreus A. nidulans A. flavus Azole resistance A. fumigatus A. niger Species of Aspergillus causing IA Species A. fumigatus Voriconazole RCT (MITT) TransNet (surveillance) MSG multicentre study 85 (77%) 136 (74%) 171 (67%) A. flavus 7 16 41 A. niger 9 13 14 A. terreus 6 10 8 Other 3 8 4 167 16 18 Not speciated Multiple 28 Filamentous fungi and antifungal drug activity Highly active Very active Active Inactive Amphotericin B Caspofungin Voriconazole % frequency Posaconazole 75 5 5 2 1 10 1 1 Arguments for not using voriconazole 1. Amphotericin B is a broader spectrum agent – No 2. AmBisome is equivalent to voriconazole in IA Randomised study of invasive aspergillosis with voriconazole versus amphotericin B 391 pts received either 1) Voriconazole 4 mg/d BID (after loading) for 12wks (or OLAT) or 2) AmB 1.0 mg/kg/d for 12wks (or OLAT) mITT analysis Success (%) Severe AEs (%) Renal tox (%) Died (all) (%) Vori 53 13 1 29 AmB 32 } 21% 24 10 42 } 13% Herbrecht, Denning et al, NEJM 2002;347:408 Survival after primary Rx with amphotericin B or voriconazole Survival (percent) 100 80 60 40 Voriconazole Amphotericin B 20 0 0 2 4 6 8 Number of patients at risk 144 131 125 117 111 133 117 99 87 84 Overall logrank test p=0.015 10 12 Weeks 107 80 102 Voriconazole 77 Amphotericin B Herbrecht, Denning et al, NEJM 2002;347:408 Impact of second line treatment after voriconazole versus amphotericin B Initial randomised Rx only Success (CR+PR)/Total (%) Voriconazole Ampho B 51/99 (51) 1/26 (4) Patients who switched Rx Lipid Ampho B Itraconazole Combination 25/52 (48) 5/14 (36) 11/17 (65) 0/1 Reason for switch Intolerance 8/16 (50) Insufficient clinical response 5/19 (26) Chronic suppression 11/14 (79) Overall success 76/144 (53) 41/107 (38) 14/47 (38) 18/38 (50) 0/9 27/72 (38) 4/21 (19) 6/10 (60) 42/133 (32) Patterson et al, Clin Infect Dis 2005;41:1448 Randomised study of invasive aspergillosis with Amphocil versus amphotericin B 174 pts received either 1) Amphocil 6 mg/d for >2wks after symptoms gone or 2) AmB 1.0 – 1.5 mg/kg/d >2wks after symptoms gone 70/174 (40%) in high risk (HSCT, liver Tx, AIDS, brain) ITT analysis Amphocil AmB Success (%) Tox (%) 13 83 15 83 Renal tox (%) Died (due to IA)(%) 23 59 (22) 41 67 (20) Bowden et al Clin Infect Dis 2002;35:359 Randomised study of invasive aspergillosis with 2 doses of AmBisome 339 pts randomised to receive either 1) L-AmB 3 mg/d for 2+wks (169 randomised; 107 in MITT) or 2) L-AmB 10 mg/d for 2+wks (162 randomised; 94 in MITT) 44/201 (22%) high risk (HSCT, AIDS) MITT analysis L-AmB 3 CR + PR 50% Stop Rx 20% Renal tox 14% Died 28% L-AmB 10 46% 32% 31% 41% Cornely et al, Clin Infect Dis 2007;44:1289 AmBiload trial results Response LAmB 3 mg/kg (n = 107) LAmB 10 mg/kg (n = 94) Survival L-AmB 3 mg/kg L-AmB 10 mg/kg Overall Response P = NS 50 40 30 50 % 20 46% p = 0.089 10 0 End of Treatment Weeks Cornely et al, Clin Infect Dis 2007;44:1289 Denning, CID 2007:45:1106 AmbiLoad study favours Ambisome compared to voriconazole because of better responding patient population, earlier diagnosis and possibly softer response criteria Denning, CID 2007:45:1106 Herbrecht et al, NEJM 2002:347:408 Open study of invasive aspergillosis with caspofungin as primary therapy 61 pts with chemotherapy or auto HSCT received Caspofungin 70 then 50mg IV daily 33% response rate Survival by day 84 = 33/61 (54%) Viscoli et al, JAC 2009;64:1274 Herbrecht at al, New Engl J Med 2002:347:408-15 Open study of invasive aspergillosis with caspofungin as primary therapy 42 pts with allo HSCT , 24 eligible, Rx Caspofungin 70 then 50mg IV /d Unrelated donors in 16 patients; acute or chronic GVHD was present in 15, 12 patients were neutropenic (<500) at baseline, Median duration of caspofungin treatment was 24 days. At EOT, 10 (42%) had complete or partial response, 12 (50%) had progressing disease. At 12 wks, 8 patients (33%) had complete or partial response. Survival rates at week 6 and 12 were 79 and 50%, respectively. Herbrecht et al, BMT 2010; 45:1227 Herbrecht at al, New Engl J Med 2002:347:408-15 Impact of voriconazole in real life Nivoix et al, Clin Infect Dis 2008;47:1176 Voriconazole versus amphotericin B [Spectrum/activity] Favours voriconazole Much more active for IA (~20% better) Active against A. terreus Active against A. nidulans More active A. flavus Active against S. apiospermum Favours Amp B Mucorales possible Azole resistant A. fumigatus Arguments for not using voriconazole 1. Amphotericin B is a broader spectrum agent – No 2. AmBisome is equivalent to voriconazole in IA – No 3. Patient was on itraconazole prophylaxis Arguments for not using voriconazole 1. Amphotericin B is a broader spectrum agent – No 2. AmBisome is equivalent to voriconazole in IA – No 3. Patient was on itraconazole prophylaxis Prophylactic Itraconazole Glasmacher & Prentice J Antimicrob Chemother 2005; 56 (Suppl 1): i23. Increased AmB MICs after pre-exposure of A. fumigatus to itraconazole Kontoyiannis AAC 2000;44:2915 Arguments for not using voriconazole 1. 2. 3. 4. Amphotericin B is a broader spectrum agent – No AmBisome is equivalent to voriconazole in IA – No Patient was on itraconazole prophylaxis – No The patient has cerebral aspergillosis Cerebral aspergillosis and voriconazole (n=81) Schwartz et al, Blood 2005, Ruhnke personal comunication Arguments for not using voriconazole 1. 2. 3. 4. Amphotericin B is a broader spectrum agent – No AmBisome is equivalent to voriconazole in IA – No Patient was on itraconazole prophylaxis – No The patient has cerebral aspergillosis – No (beware interactions) 5. The patient might have azole resistant Aspergillus Resistance in context of invasive aspergillosis Verweij, NEJM 2007;356:1481 Azole resistance in Manchester in A. fumigatus 70 Multi-azole resistant 11% 5% Itraconazole & posaconazole resistant 60 Itraconazole resistant Fully susceptible s Number of patient cases 17% 50 7% 5% 40 3% 0% 30 0% 5% 20 7% 0% 10 0% 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 Year Howard et al, Emerg Infect Dis 2009;15:1068 Arguments for not using voriconazole 1. 2. 3. 4. Amphotericin B is a broader spectrum agent – No AmBisome is equivalent to voriconazole in IA – No Patient was on itraconazole prophylaxis – No The patient has cerebral aspergillosis – No (beware interactions) 5. The patient might have azole resistant Aspergillus – maybe 6. Major drug interactions Cytochrome P450 interactions Fluc Itra Posa Vori +++ +++ ++ ++ Inhibitor 2C19 2C9 3A4 + ++ ++ + +++ Substrate 2C19 2C9 3A4 +++ +++ + + Dodds Ashley & Alexander. Drugs Today 2006;41:393. Arguments for not using voriconazole 1. 2. 3. 4. Amphotericin B is a broader spectrum agent – No AmBisome is equivalent to voriconazole in IA – No Patient was on itraconazole prophylaxis – No The patient has cerebral aspergillosis – No (beware interactions) 5. The patient might have azole resistant Aspergillus – maybe 6. Major drug interactions – yes sometimes 7. Renal failure Arguments for not using voriconazole 1. 2. 3. 4. 5. 6. 7. 8. Amphotericin B is a broader spectrum agent – No AmBisome is equivalent to voriconazole in IA – No Patient was on itraconazole prophylaxis – No The patient has cerebral aspergillosis – No (beware interactions) The patient might have azole resistant Aspergillus – maybe Major drug interactions – yes sometimes Renal failure – only IV therapy needed for any duration My patient is a young child and I am worried about blood levels Voriconazole levels in children Pasqualotto et al, Arch Dis Child 2008;93:578 Combination therapy – invasive aspergillosis Retrospective AmB failures Most HSCT 30/47 proven IA Multivariate analysis P=0.008 for combination and survival Marr et al, Clin Infect Dis 2004:39:797 Arguments for not using voriconazole 1. 2. 3. 4. 5. 6. 7. 8. Amphotericin B is a broader spectrum agent – No AmBisome is equivalent to voriconazole in IA – No Patient was on itraconazole prophylaxis – No The patient has cerebral aspergillosis – No (beware interactions) The patient might have azole resistant Aspergillus – maybe Major drug interactions – yes sometimes Renal failure – only IV therapy needed for any duration My patient is a young child and I am worried about blood levels – yes use 7mg/Kg BD (200mg BD orally) and consider combination therapy with an echinocandin and measure levels Choice of antifungal for aspergillosis Priority sequence • Voriconazole (unless drug interaction) • AmBisome 3mg/Kg (if not ‘nephro-critical’) OR caspofungin/micafungin (if not neutropenic) 3. Posaconazole (oral only, if no drug interactions) 4. Itraconazole When not to use voriconazole as primary therapy? Absolute contraindications • Drug interactions (ie rifampicin, carbamazepine, phenytoin etc) • Voriconazole used as prophylaxis (but not itraconazole or posaconazole) • Resistance to voriconazole (esp zygomycosis, A. lentulus or azole resistance) Relative contraindications • Renal failure (IV only) • Young children (need higher dose ?+ other agent) • Severe hepatic dysfunction • Interacting drugs (ie sirolimus) Random voriconazole concentrations in adults receiving 3mg/Kg BID Log 10 [Concentration (µg/L)] 100,000 Possible toxicity 10,000 1000 100 Very small children may metabolise voriconazole very fast and need dose escalation to ?7-10mg/Kg BID or 200mg BID 10 1 0 70 140 210 280 days after first dose Data from Denning et al, Clin Infect Dis 2002;34:563 Another challenge – immune reconstitution Day 0 Day 7 Miceli, Cancer 2007;110:112; Caillot Eur J Radiol 2010;74:e172 Rapid neutrophil recovery & invasive aspergillosis = bleeding from the lung and usually death Todeschini et al, Eur J Clin Invest 1999;29:453 Immune reconstitution in invasive pulmonary aspergillosis, in AIDS Patient HB Day +14, CD4 cells 84/uL Patient HB Day +42, after AmB and ITZ Sambatakou, Eur J Clin Microbiol Infect Dis 2005;24:628 Immune reconstitution in invasive pulmonary aspergillosis, in AIDS Patient HB Day +64, CD4 cells 340/uL, on VRC Patient HB Day +87, day of death Sambatakou, Eur J Clin Microbiol Infect Dis 2005;24:628 Conclusions • Voriconazole is the treatment of choice for invasive aspergillosis • For those with toxicity, significant drug interactions or azole resistance, an echinocandin or lipid AmB is appropriate • Current treatments are partially successful but more oral therapies are needed • Immune reconstitution poorly understood, but probably important • Opportunities for immune therapies going forward 13 years and counting Over 2M pages read monthly in >125 countries Supported by the Fungal Research Trust – 20 year anniversary in 2011