Cushing’s, Adrenal Insufficiency and
Other Glucocorticoid Related Issues
Family Practice Residency Program
Waterloo, IA
September 11, 2013
Janet A. Schlechte, M.D.
Disclosure of Financial Relationships
Janet A. Schlechte, M.D.
has no relationships with any
proprietary entity producing
health care goods or
services consumed by or
used on patients.
Objectives
• Approach to glucocorticoid
excess
• Management of adrenal
insufficiency
• Peri-op management of
glucocorticoids
• Steroid taper
Cushing’s Syndrome Causes
• ACTH secreting pituitary tumor
• Adrenal adenoma/carcinoma
• Ectopic ACTH production
• Exogenous glucocorticoid
Classic Features of
Cushing’s
• Centripetal obesity
• Violaceous striae
• Proximal muscle weakness
• Amenorrhea
• Thin skin
• Bruising
Other Features of Cushing’s
• Hypertension
• Glucose intolerance
• Diabetes
• Hypokalemia
• Bone loss
Causes of Cushing’s
Syndrome
• ACTH secreting pituitary
tumor
• Adrenal adenoma/carcinoma
• Ectopic ACTH production
• Exogenous glucocorticoid
Pituitary versus Adrenal Cushing’s
Ectopic ACTH Secretion
• Severe hypokalemia
• Metabolic alkalosis
• Muscle weakness
• Few of the classic stigmata
• Hyperpigmentation
Cushing’s Syndrome
• Rare disorder
• How often will it
present in the
primary care setting?
• Many people complain of
weight gain and bruising but
few have Cushing’s
• Even astute clinicians should
screen for glucocorticoid
excess
Screening Tests
• 24 hour urine cortisol
• 1 mg dex test
• 11 p.m. salivary cortisol
24 Hour Urine Cortisol
• Inconvenient but most
sensitive
• May need to do more than
one unless results are 2-3x
normal
• Occasional false positives
16
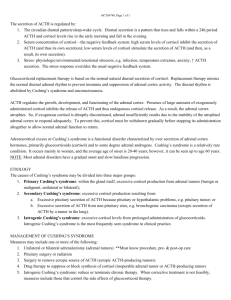
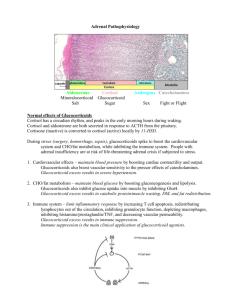
Diurnal Variation of
Cortisol
14
Cortisol
12
10
Pre-Dex
8
6
4
Post-Dex
2
2400
0500
1000
Time
1500
2000
1 mg Dex Test
• 1 mg dexamethasone at 11
p.m. and measure 8 a.m.
cortisol the next day
• Healthy subjects will have
cortisol <2 µg/dl
1 mg Dex Test
• false positives
- dilantin
- obesity
- estrogen
- stress
- depression
A 30 y.o. woman has gained 20
pounds over the last six months.
She has also noted leg swelling
and her blood pressure is
harder to control. She takes
HCTZ and a BCP.
B/P 140/100, BMI 35, bruises
on legs, buffalo hump, pale pink
striae.
• She has read about
Cushing’s syndrome and
is worried about a pituitary
tumor
• Potassium 3.8, A1C 5.6%,
CBC nl
• She takes 1 mg of dex at
11 p.m. and an 8 a.m.
cortisol the next day is
10 µg/dl.
• Does she have Cushing’s?
• She collects a 24 hour
UFC and the result is
53 µg/dl (<50)
• Does she have
Cushing’s?
A 40 y.o. man has poorly
controlled hypertension. His
weight has increased by 50
lb in the last year. He has
bright purple striae and
significant muscle weakness.
A 1 mg DST shows a cortisol
of 20 so screening test is
positive.
• To rule out a false positive do
confirmatory test
• He collects a 24 hour UFC
and the value is 350 µg/dl
(<50)
• Test is positive – he has
Cushing’s
• Now what?
When cortisol excess is
confirmed draw
ACTH
ACTH
Pituitary tumor
Adrenal tumor
Ectopic
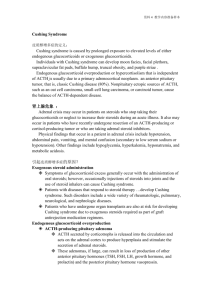
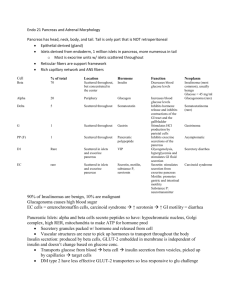
Glucocorticoid Excess
Screening Test
Normal
Abnormal
Confirm Test
Stop
Normal
Abnormal
Get ACTH
Undetectable
Adrenal
Stop
Elevated
Pituitary
Ectopic
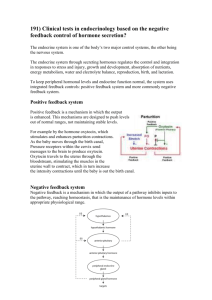
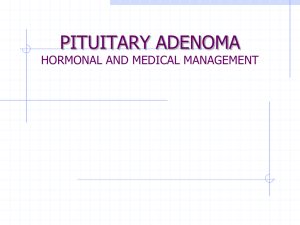
Do DST to differentiate
ACTH
Cortiso
l
Pituitary
Hyperfunction
ACTH
Cortiso
l
Adrena
l
Tumor
ACTH
Cortiso
l
Ectopic
Production
Urinary free cortisol
baseline
300 µg
989 µg
4034 µg
2 mg
180
991
4000
8 mg
40
990
3989
ACTH
undet.
A 41 y.o. collapsed on the golf
course in August. For 6 months
he has been tired with
intermittent nausea, abdominal
pain and deterioration of his golf
game. In the ER his BP was 60/with a pulse of 130. He has a
deep tan, pigmented buccal
mucosa, a small thyroid and a
normal neuro exam.
In The ER
• Sodium
• Potassium
• Chloride
• CO2
• Creatinine
• Glucose
125
6.4
98
18
1.4
75
Features of Primary AI
• Hyperpigmentation
• Fatigue and weakness
• Hypotension
• Postural dizziness
• Abdominal pain
• Weight loss
Causes of Primary
Adrenal Insufficiency
• Autoimmune
• Adrenal hemorrhage
• Granulomatous disease
• Your working diagnosis is
primary adrenal
insufficiency.
• How do you confirm your
suspicion?
• Cortrosyn stimulation test
- Measure plasma cortisol
before and 1 hour after IM
injection of 250 µg ACTH
(cortrosyn)
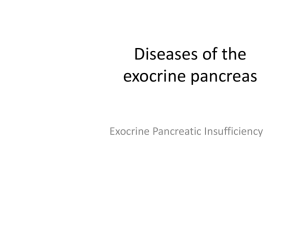
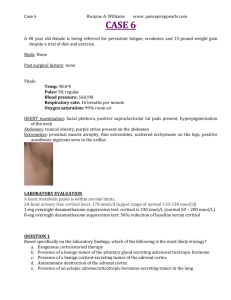
Short Cortrosyn Stimulation Test
Cortisol
Normal
1° AI
• After cortrosyn stimulation test
begin steroid replacement.
• Little practical reason to start
dexamethasone before
cortrosyn.
After the cortrosyn test the IV
saline is continued and you
give the 100 mg of
hydrocortisone. One hour
later the lab calls with the
cortisol results.
• Basal cortisol 0.1 µg/dl
• Stimulated cortisol 0.1 µg/dl
What if the results were
• Basal cortisol 9 µg/dl
• Stimulated cortisol 25 µg/dl
Classical Glucocorticoid
Equivalents
Daily Replacement Doses
5 mg
20-25 mg
Prednisone
Hydrocortisone
0.75 mg
Dexamethasone
37.5 mg
Cortisone acetate
More Physiologic
Equivalents
Daily Replacement Doses
5 mg
Prednisone
10-15 mg
Hydrocortisone
0.75 mg
Dexamethasone
Treatment Guidelines
• Monitor therapy clinically
and with electrolytes.
• Can’t use ACTH or cortisol
to monitor therapy.
• Consider other autoimmune
disease.
Long-Term Therapy
• Hydrocortisone (10-15 mg/day)
• Start with hydrocortisone and
add florinef as needed.
• Florinef (0.05-0.1 mg/day)
• Educate patient about use
of steroid during “stress”
• Yearly follow-up
Stress dose?
• Pulling wisdom teeth
• Colonoscopy
• Endometrial biopsy
• Flu with aches and pains
Stress dose?
• CABG
• Hip replacement
• Final exams
• Death in the family
A 45 y.o. woman with RA has
been treated with 10 mg of
prednisone for 3 years. She
will undergo laparoscopic
surgery in 2 days. Her
surgeon wants you to write
pre-op orders.
• Pituitary adrenal axis is
suppressed
• ACTH due to exogenous
glucocorticoid
• Stopping glucocorticoid
and/or stress of surgery
could lead to adrenal crisis
Peri-Operative
Corticosteroid Coverage
• Minor surgical stress
- usual dose day of procedure
• Moderate surgical stress
- 50 mg HC day of procedure
then resume usual dose
Ann Surg 219:416, 1994
Peri-Operative
Corticosteroid Coverage
• Major surgical stress
- 100 mg HC on day of procedure
- 50 mg HC on post-op day 1
• Resume usual dose unless
clinical condition deteriorates
Ann Surg 219:416, 1994
• Avoid too much glucocorticoid
• After a stress dose rapidly
resume the replacement dose
• Don’t use cortisol or ACTH to
try to monitor therapy
A 60 y.o. man has taken 60
mg of prednisone daily for 6
months for anterior ischemic
optic neuropathy. His
ophthalmologist has seen no
improvement and wants to
stop the steroid.
The Dilemma
• Stopping the drug will lead to
secondary adrenal insufficiency
• He has muscle weakness and
weight gain and his T score is
-2.9. The glucocorticoid needs
to be stopped as rapidly as
possible
Taper
Option # 1
January 1
January 15
January 30
February 1
February 15
March 1
60 mg
40 mg
20 mg
10 mg
5 mg
Off
Taper
Option # 2
January 1
January 15
February 1
March 1
April 1
60 mg
60 mg q.o.d.
30 mg q.o.d.
10 mg q.o.d.
Off
Taper
Option # 3
January 1
60 mg
January 2
10 mg
February 1
9 mg
March 1
8 mg
April 1
7 mg
May 1
6 mg
etc. until off
Questions to Ask
• What is the reason for the
taper?
• Is it to avoid recurrence of
disease?
• Is it to avoid adrenal crisis?
Effect of Dose of Hydrocortisone
on Mortality
0<HC<20
RR
1.3
95% CI
0.7-2.6
p
ns
20<HC<25
1.4
0.6-3.3
ns
25<HC<30
1.6
1.1-2.4
.014
HC>30
2.9
1.4-5.9
.003
JCEM 94:4216, 2009
Take Home Points
• Remember glucocorticoid
equivalencies
• Use stress doses sparingly
• When HPA axis is suppressed,
taper slowly beginning at a
maintenance dose
A 42 y.o. with a history of
chronic back pain has
severe fatigue and the lab
pages you because his
cortisol is 1.0 and his TSH is
1.4.
One of your patients takes 5 mg
of prednisone daily after an
organ transplant. She is having
her wisdom teeth pulled
tomorrow morning and calls to
find out what to do about her
prednisone since she will be
NPO.
 0
0